1. Background
Medical education is rapidly changing due to various factors like changes in the health care environment, changes in the role of physicians, rapid changes in medical science, altered societal expectations, and diversity of pedagogical techniques. Many online platforms are now available for medical students; however, not every student is using it to its full extent. During the era of the COVID-19 pandemic, due to the extended period of lockdown, online medical education has become almost mandatory for all health science students and institutions.
E-learning has a well-established role in medical education and can be effective in enhancing learning. It is well accepted by the students (1-3). E-learning can be used both as a stand-alone teaching tool and in a blended learning environment where it is linked to in-person classroom teaching (4). It is beneficial for the improvement of knowledge, i.e., the cognitive domain. E-learning involving videos can be used to develop soft skills like good communication and consulting skills, which are fundamental for improving health outcomes (5).
During the COVID-19 pandemic, the utility of e-learning has significantly increased. We aimed to study the scenario of e-learning among undergraduate students of health science during this lockdown period.
2. Objectives
For this educational research, our objectives included identifying students using e-learning packages as a method of study before the pandemic, identifying the e-learning scenarios during the COVID-19 pandemic, recognizing the most common method/s used by institutions for online learning, and finding out the perception of students about the change in the teaching-learning methods in their institution.
3. Methods
This was a questionnaire-based anonymous online survey. All undergraduate students of government and private health science institutions of various states across India whose education was affected by the pandemic and were willing to participate in the survey were included in the study. Students who did not give their consent were excluded from the study. A cross-sectional study was conducted from April to June 2020 at a medical college in Western Maharashtra, India. The sample size was calculated, assuming that 50% of students were using e-learning packages, with an allowable error of 5% and a confidence level of 95%. The calculated sample size was 384 using Epi Info™ (version 7.2) software. The response rate in online surveys is unpredictable. Therefore, we circulated the forms in various college groups and received responses from 914 students. Nine out of the 914 students who responded to the survey did not give their consent. Hence, the final sample size was 905. Institutional ethics committee clearance was taken (Ref. No. DYPV/EC/502/2020). Written informed consent was also obtained from the participants.
The online survey was carried out using Google forms. The questionnaire was prepared in three sections: Sociodemographic and academic details, Utilization of commercially available e-learning packages for learning by students before the pandemic, and teaching-learning activities during the COVID-19 pandemic carried out by the institutions.
The questionnaire on the utilization of commercially available e-learning packages included the use of any e-learning program, duration of use, number of programs they were enrolled in, the usefulness of e-learning programs in clarifying their concepts, frequency of learning, etc. This was designed to identify the students who were already conversant with e-learning and get an idea of how e-learning benefited them in clarifying their concepts using a five-point Likert scale.
The next section of the questionnaire was on teaching-learning activities during the COVID-19 pandemic, which included the mandatory use of institutional e-learning after lockdown, availability of gadgets and connectivity, preferred method of learning by students, the feasibility of e-learning provided by their institution, and the satisfaction level among students about clarifying concepts and improving communication skills by institutional e-learning activities. One open-ended question was asked to give suggestions to improve institutional e-learning activities.
These different sections of the questionnaire helped us to identify the role of e-learning during the pandemic and judge the quality of academic e-learning programs and students’ perceptions about e-learning in medical education. The questionnaire was e-validated by a pilot study. Reliability was obtained in the form of internal consistency (Cronbach’s alpha of 0.74), for important questions on the satisfaction level of students with institutional e-learning activities.
Data analysis was done using Epi Info™ (version 7.2) software. Qualitative data were presented as numbers and percentages and 95% Confidence Interval(CI) and quantitative data as mean and Standard Deviation (SD).
4. Results
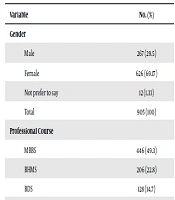
The total participants approached for the online survey were 914; however, 1% (n = 9) of the participants did not give consent for participation. Hence, the non-response rate was 1%. The responses were recorded for 905 participants, of whom 29.50% (n = 267) were males, and 69.17% (n = 626) were females. The mean (SD) age of the participants was 20.53 (1.78) years. The participants belonged to different health science courses: 49.30% (n = 446) from the MBBS curriculum and 22.80% (n = 206) from the BHMS curriculum. The majority of the participants were from private colleges (n = 740; 81.77%). The detailed sociodemographic data are shown in Table 1.
Table 1.
Sociodemographic Details of Students
| Variable | No. (%) |
|---|---|
| Gender | |
| Male | 267 (29.5) |
| Female | 626 (69.17) |
| Not prefer to say | 12 (1.33) |
| Total | 905 (100) |
| Professional Course | |
| MBBS | 446 (49.3) |
| BHMS | 206 (22.8) |
| BDS | 128 (14.7) |
| BPTH | 78 (8.6) |
| BOPTOM | 38 (4.2) |
| Others | 9 (0.4) |
| Total | 905 (100) |
| Type of Organization | |
| Government | 165 (18.23) |
| Private | 740 (81.77) |
| Total | 905 (100) |
Table 2 describes the utilization of commercially available e-learning programs by students before the COVID-19 pandemic and their perception of clarifying concepts. It was observed that 50.83% (n = 460) of the students were using some forms of e-learning programs before the COVID-19 pandemic. Besides, 55.4% (n = 332) of the participants used e-learning daily, and 6.7% (n = 40) used either during exams or for clarifying doubts. This showed that the remaining students were either using e-learning occasionally or with less frequency. The majority of the students (n = 209; 45.43%) used free versions; 33.48% (n = 154) used paid versions, and 21.09% (n = 97) of the students used both free and paid versions. These e-learning programs were found by the majority of the students to be useful for clarifying their concepts; however, 11.52% (n = 53) were not able to decide on their utility. Very few students did not find them useful. Teaching-learning activities by institutions during the COVID-19 pandemic are shown in Table 3.
Table 2.
Utilization of Commercial e-learning Programs by Students Before COVID-19 Pandemic
| Variable | No. (%) | 95% Confidence Interval |
|---|---|---|
| Use of commercial e-learning programs | ||
| Yes | 460 (50.83) | 47.57 -54.08 |
| No | 445 (49.17) | 45.92 -52.43 |
| Total | 905 (100) | |
| Commercial e-learning program versions | ||
| Both (free + paid) | 97 (21.09) | 17.61 -25.05 |
| Paid | 154 (33.48) | 29.32 -37.91 |
| Free | 209 (45.43) | 40.94 -50 |
| Total | 460 (100) | |
| Duration of using any e-learning program | ||
| Less than one month | 154 (33.47) | 29.32 -37.91 |
| One to three months | 162 (35.22) | 30.99 -39.69 |
| Three to six months | 44 (9.57) | 7.2 -12.6 |
| More than six months | 100 (21.74) | 18.21 -25.73 |
| Total | 460 (100) | |
| Usefulness of commercial e-learning programs in clarifying concepts | ||
| Not useful at all | 2 (0.43) | 0.12 -1.57 |
| Not useful | 10 (2.17) | 1.19 -3.96 |
| Undecided | 53 (11.52) | 8.92 -14.76 |
| Useful | 232 (50.44) | 45.88 -54.98 |
| Very useful | 163 (35.44) | 31.2 -39.91 |
| Total | 460 (100) |
Table 3.
Teaching-Learning Activities by Institutions During COVID -19 Pandemic
| Variable | No. (%) | 95% Confidence Interval |
|---|---|---|
| Mandatory use of institutional e-learning during COVID -19 Pandemic | ||
| Yes | 644 (71.16) | 68.12 -74.02 |
| No | 261 (28.84) | 25.98 -31.88 |
| Total | 905 (100) | |
| Did the institute conduct e-learning before COVID-19 Pandemic? | ||
| Yes | 194 (30.12) | 26.71 -33.78 |
| No | 450 (69.88) | 66.22 -73.29 |
| Total | 644 (100) | |
| Types of institutional e-learning methods | ||
| LMS +Google classroom +Zoom meet +Google meet | 233 (36.18) | |
| Google meet +Zoom meet | 180 (27.95) | |
| LMS +Google meet +Zoom meet | 87 (13.51) | |
| LMS | 47 (7.3) | |
| Google classroom | 32 (4.97) | |
| LMS +Google classroom | 32 (4.97) | |
| Google meet+ Zoom meet+ Google classroom | 23 (3.57) | |
| Others (MOOC, Microsoft teams, etc.) | 10 (1.55) | |
| Total | 644 (100) | |
| Availability of gadgets and internet connectivity | ||
| Yes | 472 (73.29) | 69.74 -76.56 |
| No | 172 (26.71) | 23.44 -30.26 |
| Total | 644 (100) | |
| E-learning has flexibility and autonomy | ||
| Yes | 445 (69.1) | 65.43 -72.55 |
| No | 199 (30.9) | 27.45 -34.57 |
| Total | 644 (100) | |
| Provision of support and training for e-learning by institutions | ||
| Yes | 400 (62.11) | 58.37 -65.83 |
| No | 244 (37.89) | 34.02 -41.48 |
| Total | 644 (100) | |
| Teaching-learning methods preferred by students | ||
| Both (traditional + e-learning) | 325 (50.47) | 46.61 -54.31 |
| Traditional Classroom methods (in-person classes conducted by teachers) | 255 (39.6) | 35.89 -43.42 |
| E-Learning | 64 (9.93) | 7.86 -12.49 |
| Total | 644 (100) | |
| Feasibility of e-learning provided by institutions | ||
| Not feasible at all | 25 (3.88) | 2.64 -5.67 |
| Not feasible | 70 (10.87) | 8.69 -13.51 |
| Undecided | 131 (20.34) | 17.41 -23.62 |
| Feasible | 309 (47.98) | 44.15 -51.84 |
| Very feasible | 109 (16.93) | 14.23 -20.02 |
| Total | 644 (100) | |
| Satisfaction level of students with institutional e-learning programs in clarifying concepts | ||
| Completely Satisfied | 67 (10.4) | 8.28 -13 |
| Satisfied | 319 (49.53) | 45.69 -53.39 |
| Undecided | 131 (20.35) | 17.41 -23.62 |
| Not Satisfied | 95 (14.75) | 12.22 -17.7 |
| Not Satisfied at all | 32 (4.97) | 3.54 -6.93 |
| Total | 644 (100) | |
| Satisfaction level of students with institutional e-learning programs in improving communication skills | ||
| Completely satisfied | 50 (7.76) | 5.94 -10.09 |
| Satisfied | 270 (41.93) | 38.17 -45.77 |
| Undecided | 166 (25.78) | 22.55 -29.29 |
| Not satisfied | 115 (17.86) | 15.09 -21 |
| Not satisfied at all | 43 (6.67) | 4.99 -8.87 |
| Total | 644 (100) | |
| E-assessment conducted by institutions | ||
| Yes | 511 (79.35) | 76.23 -82.48 |
| No | 133 (20.65) | 17.52 -23.77 |
| Total | 644 (100) | |
| Satisfaction level of students with institutional e-assessment | ||
| Completely satisfied | 68 (13.31) | 10.63 -16.53 |
| Satisfied | 276 (54.01) | 49.68 -58.29 |
| Undecided | 103 (20.16) | 16.91 -23.85 |
| Not satisfied | 49 (9.58) | 7.33 -12.45 |
| Not satisfied at all | 15 (2.94) | 1.79 -4.79 |
| Total | 511 (100) |
The results of the survey revealed that it became mandatory for 71.16% (n = 644) of the students to use institutional e-learning. Only 30.12% (n = 194) of the students were exposed to regular institutional e-learning before lockdown. Gadgets and internet connectivity were already available for many students (n = 472; 73.29%). Half of the students (n = 325) preferred both traditional and e-learning methods, whereas only 9.93% (n = 64) preferred exclusively e-learning.
We surveyed the feasibility of implementing institutional e-learning during the pandemic on a five-point Likert scale, with 5 being “Very feasible“ and 1 being ‘Not feasible at all’. The feasibility of e-learning by the institution was appreciated by most students; 47.98% (n = 309) rated it as ‘Feasible’ and 16.93% (n = 109) as ‘Very Feasible’. Moreover, 62.11% (n = 400) of the students had been trained on the use of institutional e-learning methodology. This helped the students to use technology for their academics during the COVID- 19 pandemic, especially for non-users or seldom users.
The level of satisfaction with concept clarification was lower by institutional e-learning (60%; n=386/644) than by commercially available e-learning programs (85%; n = 395/460). However, the majority of them were satisfied with institutional e-learning programs in improving communication skills. Besides, 79.35% (n = 511) of the students surveyed had been prepared for institutional e-assessment, 13.31% (n = 68) of whom were completely satisfied, and 12% (n = 64) were not satisfied with e-assessment.
Some of the suggestions given by students to improve institutional e-learning activities were the improvement of the teaching-learning process, including teachers’ training, more interactivity, usage of Powerpoint presentations with audios (n = 140), internet connectivity, and infrastructure issues (n = 99). Improvement in the assessment methods and increases in frequency were also suggested (n = 25). A few students (n = 5) pointed out the lack of skill training (psychomotor domain) on the e-learning process.
5. Discussion
In this online survey, the majority of the participants were females. This shows that female students more preferred to participate in the survey. The mean age of the students was 20.53 (SD 1.78) years, as most of them were in the age group of 20-25 years. Since the number of seats in the medical curriculum was more than that of other fields like BHMS, the maximum responses were obtained from medical students. The significantly higher number of participants from private colleges can be explained again by circulation bias. The limitation of representation from government colleges could be due to their involvement in the management of the COVID-19 pandemic.
E-learning has been witnessing an unprecedented expansion as an opportunity for higher education (6). This is also seen by our survey that 50.83% (n = 460) were already using commercial e-learning programs of whom the majority was using free versions. This shows that paid versions were not easily accessible and affordable by many students. Free versions were used by many students and also by students who were already using paid versions to compare the two different platforms of learning. It was observed that 33.47% (n = 154) of the students commenced utilizing e-learning only recently. This shows that e-learning was prevalent among health science students, but its’ usage increased and became mandatory during the COVID-19 pandemic.
Almost 85% (n = 395) of the participants found it useful for clarifying their concepts. A similar study by Warnecke et al. showed that 54% of students agreed that e-learning was good in understanding the concepts (4). The reason for this was the advancement in technology, innovative e-learning techniques, and self-motivated students opting for e-learning due to the flexibility of e-learning programs. A study conducted by Ullah et al. showed that 71% of students agreed that access to education increased through online learning. However, 18% of students could not decide, and 10% did not agree with it (7). This is in line with our findings.
It was found that 30.12% (n = 194) of the students had been provided by institutional e-learning before the COVID -19 pandemic. However, it became mandatory to use this pedagogy by the majority of the students (n = 644; 71.16%). The various e-learning tools provided were synchronous, like zoom meeting and G-meet, and asynchronous, like sharing resource material through the Learning Management System (LMS) and Google classroom. Students preferred the blending of both synchronous and asynchronous e-learning methods. This is in line with a study by Dhir et al (8).
Gadgets and internet connectivity were available to 73.29% (n = 472) of students, although 26.71% (n = 172) did not have this connectivity. This could be one of the drawbacks of e-learning activities as these students would have missed their academics. This point was brought out in some recommendations given by the students. Slow computers and poor internet connections discouraged the use of e-learning (7). For effective e-learning through LMS, good access to the internet, and improved broadband speed are essential (9).
It was observed that most students preferred the blending of e-learning and traditional learning. This is in line with other studies (4, 8). The blended learning method has the advantages of sharing resources online and utilizing valuable face-to-face teaching time optimally. Approximately 9.93% (n = 64) of the students preferred an exclusive e-learning method as the mode of learning, whereas e-learning with the traditional method was preferred by 50.47% (n = 325), and only traditional classrooms were preferred by 39.60% (n = 255). This demonstrated that only e-learning was not a preferred method in health science education. The lack of direct interaction with teachers, peers, and patients, along with the absence of an educational environment, could be the reason for the same. A similar study by Al-Adwan et al. concluded that the implementation of e-learning as a supplement to traditional face-to-face lectures enhanced student’s learning experience (10). The reason for preferring e-learning was the flexibility and autonomy provided by this program. Almost 69.10% (n = 445) agreed upon this issue. Other studies are also in line with our findings (11).
Most of the students (n = 418; 65%) rated institutional e-learning as feasible. However, around 20.34% (n = 131) were undecided and 15% (n = 95) could not find it feasible. This was proved by Vitoria et al., who revealed a 100% feasibility (11). The disparity in percentages could be explained by their low sample size and connectivity issues raised by our study participants. Support and training regarding institutional e-learning were received by 62.11% (n = 400) of students. This would have helped the students to use technology for their academics during the COVID-19 pandemic, especially nonusers or seldom users.
It was observed that the students were more satisfied with commercial e-learning packages than with institutional e-learning for clarifying concepts. This difference was attributed to the professionalism of e-programs designed, trained faculty, better audio-visual effects, good information technology support, and self-motivation of students for commercial packages. This was brought out by students in their suggestions on institutional e-learning programs. However, the COVID -19 pandemic was like a disaster for the education system. Both teachers and students were not prepared for this sudden change in the academic schedule and pedagogy. E-learning has provided a platform for teaching-learning activities during the COVID 19 pandemic.
E-assessment is still under emerging phases in the health science assessment system. Formative assessments using MCQS designed on Google forms, survey monkey, podcasts, gaming apps like Kahoot, etc. are under exploration by medical faculties. However, there is limited usage of e-assessment in health science education to date.
The limitation of the study: This was a rapid online appraisal to figure out the scenario of e-learning during the COVID-19 pandemic. As it was an online survey, we had a limited duration of circulation, a limited number of questions, and limitations in in-depth reasoning of some questions. The students who were inclined to and already using e-learning programs were more likely to respond to surveys on e-learning activities.
In conclusion, the COVID-19 pandemic has changed the scenario of the teaching-learning process. The study tried to identify what changes have occurred and how the students perceive this changed environment. The utilization of e-learning programs in our study revealed that half of the students were already using this technology before the COVID-19 pandemic. One-third of them started using e-learning programs only during the pandemic. The commonest method preferred by the students was blended learning. The students were satisfied with e-learning for concept clarification and communication skills. However, it has limitations for psychomotor skill training and e-assessment. Thus e-learning is beneficial during emergencies like the COVID-19 pandemic. However, exclusive e-learning has many limitations, especially in health science courses. In the future, with the competency-based curriculum, e-learning should be incorporated with traditional classroom teaching for an optimal educational environment.