





1. Background
The novel coronavirus, severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), responsible for the COVID-19 outbreak, was first identified in China at the end of 2019 (1). The virus spread rapidly, causing significant mortality at an unprecedented rate worldwide, leading the World Health Organization to declare it a pandemic on March 12, 2020 (2). Nigeria reported its first COVID-19 case on February 27, 2020, which quickly led to an initial partial lockdown followed by a total national lockdown (3).
Ophthalmology, as both a medical and surgical specialty, requires that trainees gain comprehensive exposure in both domains to achieve expected levels of competency (4). In addition to theoretical knowledge of the eye and eye diseases, core competencies in ophthalmic residency training—highlighted in the training curricula of national and sub-regional bodies—are typically structured into four critical areas: (1) refraction skills, (2) clinical skills, (3) surgical skills, research, and (4) soft Skills acquisition (5, 6). This study evaluated the impact of the COVID-19 pandemic on these essential areas of ophthalmology training.
As countries worldwide imposed movement restrictions, most ophthalmic departments suspended elective clinical and surgical activities, limiting their practices to urgent cases only (7). This greatly impacted the provision of services and disrupted the training of ophthalmic resident doctors.
Numerous studies from different countries have examined the impact of COVID-19 on ophthalmic residency training, though most of these studies were conducted in developed economies (7-17). The majority focused on trainees’ perspectives, with only a few surveying training directors or a mix of practitioners. In Nigeria, Sarimiye et al. (18) reported on the impact of COVID-19 from the viewpoint of ophthalmology resident doctors. Despite the pandemic’s significant impact on medical education worldwide, there remains a gap in research specifically examining the perspective of ophthalmic trainers on how COVID-19 has affected ophthalmology residency training in Nigeria.
2. Objectives
This study aims to bridge this knowledge gap by exploring the experiences, challenges, and perceptions of ophthalmic trainers in Nigeria regarding the disruptions caused by the first 12 months of the COVID-19 pandemic and their implications for ophthalmology residency training. By addressing this gap, the study seeks to provide valuable insights into the specific challenges faced by ophthalmology residency programs in Nigeria during the pandemic and to identify potential strategies for mitigating similar challenges in the future. Focusing on the trainers’ perspective, our study aims to contribute to the current literature by highlighting the impact of the pandemic’s first year on ophthalmology training in Nigeria.
3. Methods
A nationwide web-based survey was conducted among ophthalmology trainers in accredited ophthalmic residency training institutions across Nigeria to capture their perspectives on the impact of the COVID-19 pandemic on ophthalmic residency training one year after the pandemic's onset in the country. The pandemic led to a nationwide lockdown and phased restrictions beginning on March 30, 2020 (3, 19).
Ethical approval for this study was obtained from the Health Research Ethics Committee of the Institute of Public Health, Obafemi Awolowo University, Ile-Ife, Nigeria (protocol number IPHOAU/12/1653, approved on April 15, 2021). Informed consent was obtained and documented electronically.
A formal sample size calculation was not applied in this study. Instead, the approach was to include all trainers in accredited institutions nationwide to ensure comprehensive representation. This inclusive approach aimed to provide a holistic view of the COVID-19 pandemic's impact on ophthalmic residency training in Nigeria, thereby offering a thorough understanding of the challenges faced and potential strategies for future resilience.
The questionnaire used in this study underwent a rigorous development process to ensure validity and reliability. This included a pre-testing phase where a sample of ophthalmology trainers reviewed the questionnaire to provide feedback on clarity and relevance. The content of the questionnaire was informed by insights from experienced ophthalmology educators and a literature review on the impact of COVID-19 on medical education. Although no pre-existing validated questionnaires directly addressed our study’s scope, these sources were used to construct a tailored, contextually relevant questionnaire. These steps were taken to enhance the questionnaire’s validity and reliability, ensuring it effectively captured ophthalmology trainers' perspectives on the impact of COVID-19 on residency training in Nigeria. Due to the limited sample size of the pilot, a formal calculation of internal consistency using Cronbach's alpha was not performed.
Respondents were from 30 training hospitals accredited by the National Postgraduate Medical College of Nigeria as of March 2021. The list of accredited institutions was obtained from the National Postgraduate Medical College of Nigeria. All 30 institutions were contacted to gather details of current trainers, and an invitation with the survey access link was sent to the personal emails of 256 trainers. Reminders were circulated via national professional social media platforms, including WhatsApp and Telegram.
The questionnaire covered key themes: Demographics, assessment of core training competencies, availability of facilities, the impact of COVID-19, and recommendations. These themes were informed by the training curricula and guidelines from the National Postgraduate Medical College of Nigeria and the West African College of Surgeons, which outline core competencies and essential areas for ophthalmology training (5, 6). The questionnaire was pilot-tested with five trainers selected from five accredited institutions across five of Nigeria’s six geopolitical zones. The final version of the questionnaire incorporated feedback from the pilot survey.
Predominantly composed of closed-ended questions, the questionnaire employed a 5-point Likert scale to assess trainers' perceptions of COVID-19's impact on ophthalmology residency training and core competency areas. Open-ended questions were included in the recommendation section to allow trainers to provide more detailed insights. Survey data was collected over five weeks (March 18 to April 21, 2021), with only one submission allowed per respondent.
Data were analyzed using IBM SPSS Statistics for Windows, version 25 (IBM Corp., Armonk, N.Y., USA). Frequency data were tabulated and utilized for descriptive statistics. Associations between categorical variables were assessed using the chi-squared test, with a P-value of less than 0.05 considered statistically significant.
4. Results
Responses were received from 162 out of the 256 trainers contacted across the 30 accredited training institutions, resulting in a response rate of 63%. These institutions were located in five of the six geopolitical zones in Nigeria; there was no accredited training institution in the North East geopolitical zone at the time of this study.
The mean age of respondents was 51.3 ± 8.6 years, with an age range of 37 to 75 years. The majority of respondents (71%) were from federal government-owned hospitals, while 20.4% and 8.6% were from state government-owned and mission/private hospitals, respectively. Respondents’ years of post-qualification experience were evenly distributed (Table 1). Additionally, most respondents were from the southern regions of the country.
| Socio-demographic Parameters | Frequency (%) |
|---|---|
| Gender | |
| Male | 69 (42.6) |
| Female | 93 (57.4) |
| Years post qualification | |
| Less than 10 years | 52 (32.1) |
| 10 - 19 years | 56 (34.6) |
| 20 years and more | 56 (33.3) |
| Institution Ownership | |
| Federal government | 115 (71) |
| State government | 33 (20.4) |
| Mission/ NGOa | 4 (1.5)10 (6.2) |
| Private | |
| Geopolitical zone | |
| North west | 30 (18.5) |
| North central | 24 (14.8) |
| North east | 0 (0.0) |
| South west | 54 (33.3) |
| South south | 20 (12.3) |
| South east | 34 (21.0) |
Distribution of 162 Respondents
Responses regarding the perceived impact of COVID-19 on the delivery of training across the core competency areas of the ophthalmic residency program (Table 2) indicated that most trainers felt COVID-19 had a moderately negative to very negative impact on all core competency areas. Notably, surgical skills transfer was the area most affected, with the highest number of respondents acknowledging the negative impact of the pandemic on this aspect of training (Table 2). Additionally, the majority of respondents (84.5%) felt that COVID-19 had a generally negative effect on their roles as ophthalmology residency trainers, with 18.5% describing the impact as very negative and 66% as moderately negative (Table 2).
| Impact on Areas of Core Competencies | Frequency (%) |
|---|---|
| How will you describe the impact of the COVID-19 pandemic on refraction training? | |
| Very severe | 19 (11.7) |
| Severe | 56 (34.6) |
| Moderate | 44 (27.2) |
| Mild | 33 (20.4) |
| Not at all | 10 (6.2) |
| How will you describe the impact of the COVID-19 pandemic on clinical skills transfer? | |
| Very severe | 22 (13.6) |
| Severe | 57 (35.2) |
| Moderate | 51 (31.5) |
| Mild | 24 (14.8) |
| Very severe | 8 (4.9) |
| How will you describe the impact of the COVID-19 pandemic on surgical skills transfer? | |
| Very severe | 46 (28.4) |
| Severe | 73 (45.1) |
| Moderate | 31 (19.1) |
| Mild | 9 (5.6) |
| Very severe | 3 (1.9) |
| How will you describe the impact of the COVID-19 pandemic on research training? | |
| Very severe | 12 (7.4) |
| Severe | 49 (30.2) |
| Moderate | 49 (30.2) |
| Mild | 36 (22.2) |
| Very severe | 16 (9.9) |
| How will you describe the impact of the COVID-19 pandemic on soft skills transfer? | |
| Very severe | 13 (8.0) |
| Severe | 49 (30.2) |
| Moderate | 48 (29.6) |
| Mild | 38 (23.5) |
| Very severe | 14 (8.6) |
| Were there facilities available during the pandemic for (‘Yes’ response) a | |
| Online learning | 125 (77.2) |
| Surgical simulation training | 31 (19.1) |
| Teleophthalmology | 32 (19.8) |
| Electronic medical records | 68 (42.0) |
| Overall, how will you describe the overall impact of the COVID-19 pandemic on your work as a trainer? | |
| Very negative | 30 (18.5) |
| Negative | 107 (66) |
| Neither negative or positive | 20 12.3) |
| Positive | 5 (3.1) |
| Very positive | 0 (0.0) |
Perceived Impact of COVID-19 on Residency Training and Use of Adaptation Tools
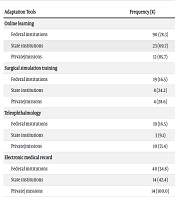
The availability of tools that could facilitate the continuation of skills acquisition and training delivery during the pandemic was also assessed (Table 3). A majority (77%) of respondents reported access to online learning facilities, while only 19% reported the availability of surgical simulation facilities. The four main tools listed in the questionnaire were consistently mentioned by respondents, and although the questionnaire allowed for open-ended responses to capture additional tools, no other tools were reported.
| Adaptation Tools | Frequency (%) | P-Value |
|---|---|---|
| Online learning | 0.427 | |
| Federal institutions | 90 (78.3) | |
| State institutions | 23 (69.7) | |
| Private/missions | 12 (85.7) | |
| Surgical simulation training | 0.393 | |
| Federal institutions | 19 (16.5) | |
| State institutions | 8 (24.2) | |
| Private/missions | 4 (28.6) | |
| Teleophthalmology | < 0.001 | |
| Federal institutions | 19 (16.5) | |
| State institutions | 3 (9.1) | |
| Private/missions | 10 (71.4) | |
| Electronic medical record | < 0.001 | |
| Federal institutions | 40 (34.8) | |
| State institutions | 14 (42.4) | |
| Private/ missions | 14 (100.0) |
Pattern of Availability Adaptation Tools During the COVID-19 Pandemic
5. Discussion
The primary aim of this study was to evaluate the impact of the COVID-19 pandemic on ophthalmology residency training in Nigeria from the perspective of ophthalmology trainers. Our findings revealed that the pandemic had a substantial negative impact on several aspects of residency training, particularly in surgical skills and clinical training. Despite these challenges, technology—such as online learning and teleophthalmology—played an essential role in helping to alleviate some of the disruptions caused by the pandemic.
Trainers play a crucial role in residency training, shaping the competencies, quality, and future capabilities of trainees (20, 21). Several survey studies from various countries have highlighted the impact of COVID-19 on ophthalmology training programs, focusing primarily on the perspectives of trainees and programmatic changes, while a few have examined the views of program directors. However, fewer studies have specifically evaluated the perspectives of trainers themselves (7-17).
The majority of trainers agreed that the COVID-19 pandemic had a substantial negative impact—rated as “a lot” or “a great deal”—on all core areas of ophthalmic residency training. Surgical skills transfer recorded the highest number of trainers expressing their perception of the pandemic’s highly negative impact. In most residency training programs, surgical skills training is one of the most challenging areas due to multiple factors (4). The pandemic led to a dramatic reduction in patient visits as a result of nationwide lockdowns and movement restrictions, which ultimately translated into fewer surgical cases. Because training programs are time-bound and residents are expected to achieve a minimum level of hands-on experience with live patients, the considerable drop in patient volume during the pandemic posed significant challenges for both ophthalmic residents and trainers (18). While many residents in the early phase of their training may have gained adequate clinic-based exposure before the pandemic, surgical competency—which requires specific case numbers and hands-on practice—is often acquired in the later stages of training. Our findings raise concerns about the surgical competency of ophthalmic residents who were in their final year of training during the pandemic, as well as for early- and mid-stage trainees who had limited or no access to structured surgical simulation training.
The pandemic led to a widespread abandonment of traditional, in-person training methods in favor of digital technology across various areas of hospital care to minimize direct human-to-human interaction (22). Globally, the adoption of technology surged as institutions sought ways to mitigate the pandemic’s impact on training and service delivery (15, 16). In our study, online learning emerged as the most commonly adopted technology, with trainers reporting that their institutions implemented it to maintain some level of postgraduate ophthalmic training. Numerous studies worldwide similarly reported that online ophthalmic learning was the primary technology adopted since the pandemic’s onset, providing the advantage of flexible, device-independent access to educational resources.
A systematic review by Chasset et al. (23), which included 60 articles, found that online courses and learning tools were the most common (88%) pedagogical solutions used to sustain medical education during the pandemic. Additionally, a survey of Nigerian ophthalmology residents by Sarimiye et al. (18) reported a significant increase in resident participation in online learning opportunities compared to the pre-pandemic period, underscoring the shift toward digital learning platforms in response to COVID-19.
In our study, electronic medical records (EMR), teleophthalmology, and surgical simulators were additional tools used to address some of the challenges posed by pandemic-related restrictions. Chasset et al. (23) reported a similar trend, noting that virtual reality/surgical simulation systems and telemedicine were among the most widely adopted facilities to mitigate COVID-19's impact on medical education, particularly in surgical specialties. The majority of trainers in privately owned and mission-affiliated training institutions had access to telemedicine and EMR facilities, which helped them navigate the challenges posed by pandemic-related safety measures and restrictions.
Telehealth utilizes electronic information and technology to support remote care, an approach that became crucial during the pandemic. Ophthalmology, however, is predominantly an outpatient surgical specialty that often requires in-person contact to manage complex conditions. While telehealth has been successfully implemented in the screening of specific eye diseases, such as diabetic retinopathy and retinopathy of prematurity, its use remains limited in low- and middle-income countries (LMICs) and for managing more prevalent eye conditions like cataract, glaucoma, and acute ocular emergencies. The deployment of telemedicine requires software, equipment, and staff training, all of which entail significant financial costs. These costs can be prohibitive for publicly owned institutions in LMICs, limiting their ability to implement telehealth solutions effectively (24-26).
This study has several limitations that should be considered when interpreting the findings. One notable limitation is the reliance on self-reporting as the primary data collection method. While self-reporting provides valuable insights into participants' perspectives and experiences, it is also subject to certain limitations that may impact the accuracy and reliability of the data.
Self-reported data is prone to recall bias, as participants may have difficulty accurately recalling past events or experiences, potentially affecting their responses and introducing bias. However, we believe that recall bias in this study was minimized, as data collection was conducted when training institutions and society at large were just beginning to recover from the pandemic's most challenging period.
To enhance the validity and reliability of the self-reported data, several measures were taken. Respondents were assured of the anonymity and confidentiality of their responses, creating a secure environment for open and honest feedback. Additionally, the questionnaire was carefully designed with clear instructions and well-structured questions to minimize potential confusion or misunderstandings.
It is important to recognize that the respondents in our study were ophthalmology trainers in accredited ophthalmic residency training institutions, bringing the requisite expertise and experience to provide informed perspectives. Their professional background and active involvement in residency programs bolster the credibility of the self-reported data.
However, the reliance on self-reporting introduces inherent limitations, and caution should be exercised when interpreting the findings. Future studies could benefit from incorporating additional data collection methods, such as direct observation or objective assessments, to complement self-reports and offer a more comprehensive understanding of the COVID-19 pandemic’s impact on ophthalmic residency training.
The findings from this survey may be applicable to contexts with similar healthcare systems, training structures, and pandemic responses. However, external validity may be limited by factors such as cultural differences, variations in healthcare infrastructure, and differences in ophthalmic residency training organization across countries. Despite the potential biases associated with self-reporting, this study offers valuable insights into the impact of the pandemic on ophthalmology residency training in Nigeria.
5.1. Conclusions
The negative impact of the COVID-19 pandemic on ophthalmic residency training, as experienced by trainers in Nigeria during the first year, was substantial. Deliberate efforts are needed to compensate for lost training time and missed opportunities. A comprehensive review of residency training in Nigeria should be undertaken to address the deficiencies in training programs exposed by the pandemic.
The integration of technology into training—particularly through online learning, surgical simulation, teleophthalmology, and electronic medical records—proved valuable. These tools not only substituted for traditional training methods but also highlighted the potential for more flexible and accessible postgraduate ophthalmic education in Nigeria.
Importantly, the disparity in access to technology between trainers in publicly-owned institutions and those in private/mission institutions underscores the need for equitable access to these tools. Building on these lessons, collaborative efforts are essential to enhance the resilience of Nigeria’s healthcare system and improve the quality of postgraduate ophthalmology training.
5.2. Lay Description
The COVID-19 pandemic significantly affected ophthalmic residency training in Nigeria during its first year. A survey of 256 trainers revealed that many experienced severe disruptions in teaching essential skills, particularly surgical techniques. While some trainers utilized online learning and teleophthalmology to adapt, the overall impact on clinical education was profound. The findings highlight the challenges faced by trainers and the importance of technology in continuing education during crises.
5.3. Highlights
Severe disruption: 73.5% of trainers reported a very severe impact on surgical skills transfer due to the pandemic.
Technology utilization: 77% of trainers had access to online learning resources, helping to mitigate some training disruptions.
Training environment: Trainers in private and mission hospitals had better access to teleophthalmology and electronic medical records compared to those in public institutions.
