



1. Background
Cystic fibrosis (CF) is an autosomal recessive disorder and the most common fatal inherited disease among whites, affecting multiple organ systems, including the respiratory tract, pancreas, reproductive, and digestive systems (1, 2). The CF treatment is complex and requires continuous, lifelong care at home with polypharmacy, including pancreatic enzymes, vitamins or nutritional supplements, mucolytics, bronchodilators, nebulizers, systemic antibiotics, anti-inflammatory agents, and drugs for associated conditions or complications (3). Treatment adherence is essential in chronic disease therapies to maintain health and life expectancy, although it is often reported to be low (4). Previous reports indicate that overall adherence in children with CF is approximately 50% (5). Non-adherence has been associated with faster disease progression, incorrect assessments of treatment effectiveness, increased risk for infections and hospitalization, reduced quality of life, and increased costs (6, 7). Proper use of medications directly enhances treatment efficacy and better control of symptoms such as night attacks, cough, and weight gain (7, 8).
Medication adherence in CF is a complex issue influenced by various factors. Patient characteristics (e.g., gender, age, ethnicity, body weight, height), family and parental factors (e.g., parents' level of education, socioeconomic status, living location), and clinical factors (e.g., duration and severity of disease) are potential predictors of adherence (9-12). Factors such as the complexity of medication regimens requiring frequent daily dosing schedules, type, and number of medications can also affect patient compliance (13). Identifying adherence rates and determining barriers to medication adherence are necessary for clinicians to provide appropriate interventions.
The exact prevalence and characteristics of CF in Iran, with its Caucasian population, are unknown. UNICEF estimates that 1800 children living with CF are registered with the Ministry of Health and receive treatment (14, 15). Although numerous studies have been published on CF treatment adherence and related factors in the United States and Europe, there is a lack of data on this subject in patients with CF in Iran.
2. Objectives
This study aimed to evaluate adherence to medication regimens among children and adolescent patients with CF at a main CF center in Iran and investigate the factors affecting adherence rates.
3. Methods
3.1. Study Design and Setting
This cross-sectional study was conducted from September 2016 to October 2017 on pediatric patients with CF who were registered and attended the CF Clinic of Children's Medical Center Hospital, the main referral CF center in Iran, affiliated with Tehran University of Medical Sciences (TUMS), Tehran, Iran. The dedicated staff of this clinic includes pediatric pulmonologists, nurses, dietitians, genetic counselors, physiotherapists, respiratory therapists, and social workers. The University Review Board/University Research Council of Islamic Azad University Tehran Medical Sciences reviewed and approved both the research and ethical aspects of this study (approval number 22510303952134).
3.2. Participants
Patients with a confirmed diagnosis of CF who received at least one medication were eligible for enrollment. The exclusion criterion was refusal to participate. Written consent was obtained from parents after a full explanation of the study. Characteristics including age, sex, ethnicity, body weight, height, time of CF diagnosis, number and frequency of physician visits, any underlying diseases, list of medications, geographic area of residence, and parents' education level were recorded by a research pharmacist through face-to-face interviews with the patient in the presence of their parents. The pharmacist asked the questions and recorded the responses indicated by the respondents.
3.3. Assessment of Adherence
The 5-item Medication Adherence Rating Scale (MARS-5) questionnaire, validated in Persian (16), was used to assess adherence to commonly used medication categories in CF patients, including inhalants, systemic antibiotics, gastrointestinal agents, and nutritional supplements. The MARS-5 consists of 5 items describing non-adherent behaviors (changing dosage, forgetting to take medication, stopping medication, skipping a dose, taking less than prescribed). Patients were asked to evaluate how often they engaged in each behavior using a 5-point scale, ranging from "always" to "never" (1 - 5 points). The total scale score ranged from 5 (indicating lowest adherence) to 25 (indicating maximal adherence compliance). Patients with a MARS-5 score of 25 were categorized as having perfect treatment adherence, while those with a score of less than 25 were classified as having lower treatment adherence.
3.4. Statistical Analysis
Descriptive statistics were expressed using frequency and percentage for categorical variables and mean, standard deviation (SD), median, and interquartile range (IQR) for continuous variables. The chi-square test or Fisher exact test was used to evaluate homogeneity between the two groups of treatment adherence (lower/perfect) for qualitative variables, and Student's t-test (in the case of normality) or Wilcoxon rank-sum test (in the case of skewness) was used for continuous variables. Binary logistic regression was performed to assess the effect of several factors on the likelihood of achieving perfect treatment adherence, estimating unadjusted and adjusted odds ratios. The model included nine risk factors: Gender, age, number of drugs, duration of CF diagnosis, number of physician visits, mother’s education level, father’s education level, distance from the medical center, and body weight. Variables that were statistically significant in the univariable logistic regression analyses with P < 0.2 were entered into a multivariable logistic regression analysis as initial risk factors. These were then analyzed by multivariable logistic regression to measure the adjusted effect of risk factors on perfect treatment adherence. Statistical significance was considered as a two-sided P-value less than .05. All statistical analyses were performed using Stata 11.2 for Windows (StataCorp. 2011. Stata Statistical Software: Release 12. College Station, TX: StataCorp LP).
4. Results
4.1. Patients’ Characteristics
A total of 300 patients were enrolled, with no exclusions from the study. Most patients were male (58.67%) and aged between 1 month and 10 years (67%). Twenty-five percent of patients took more than five drugs, while 75% took five or fewer drugs. A total of 72.67% had been diagnosed with CF for up to 5 years, whereas 27.33% had been diagnosed for more than 5 years. Seventy-two percent had physician visits two times or fewer per year, and 60.67% resided in the province where the CF center was located (Tehran). For about half of the patients, the parents' education level was illiterate (50% for mothers and 53.67% for fathers). Inhalants were prescribed for 98.33% of patients, systemic antibiotics for 83.33%, gastrointestinal agents for 80.66%, and nutritional supplements for 85.66%. Table 1 summarizes the characteristics of all patients.
| Factors and Categories | Values a |
|---|---|
| Gender | |
| Female | 124 (41.33) |
| Male | 176 (58.67) |
| Age (y) | |
| 0.08 - 10 | 201 (67.00) |
| 10 - 18 | 79 (26.33) |
| 18 - 25 | 20 (6.67) |
| Number of drugs | |
| ≤ 5 | 225 (75.00) |
| > 5 | 75 (25.00) |
| Duration of CF diagnosis (y) | |
| ≤ 5 | 218 (72.67) |
| > 5 | 82 (27.33) |
| Number of physician visits | |
| ≤ Twice a year | 216 (72.00) |
| > Twice a year | 84 (28.00) |
| Mother’s education levels | |
| Illiterate | 150 (50.00) |
| High school diploma | 121 (40.33) |
| University education | 29 (9.67) |
| Father’s education levels | |
| Illiterate | 161 (53.67) |
| High school diploma | 115 (38.33) |
| University education | 24 (8.00) |
| Distance to medical center | |
| Tehran province | 182 (60.67) |
| Outside of Tehran | 118 (39.33) |
| Medication | |
| Inhalant | 295 (98.33) |
| Systemic antibiotic | 250 (83.33) |
| Gastrointestinal agent | 242 (80.66) |
| Nutritional supplement | 257 (85.66) |
| Age (y) | 7 (3 - 11.5) |
| Weight (kg) | 18.75 (11 - 27) |
| Height (cm) | 112 (88 - 137) |
General Characteristics of Participants (N = 300)
4.2. 5-Item Medication Adherence Rating Scale Score and Level of Medication Adherence
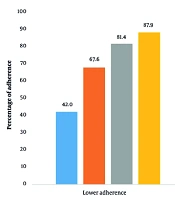
The overall mean score of the MARS-5 for all medications was 17.20 ± 5.52. The median MARS-5 score for each medication category was as follows: 25.00 (IQR, 21.00 - 25.00) for inhalants, 21.00 (IQR, 17.00 - 25.00) for systemic antibiotics, 17.00 (IQR, 9.00 - 21.00) for gastrointestinal agents, and 17.00 (IQR, 5.00 - 21.00) for nutritional supplements. Between 42.03% and 87.94% of patients with CF were lower-adherent in at least one portion of their treatment plan. Additionally, among those who received all medications, 86.91% were lower-adherent. Specifically, 42.03% of patients had lower adherence to inhalants, 67.60% to systemic antibiotics, 81.40% to gastrointestinal agents, and 87.94% to nutritional supplements. The classification of adherence to all four medication categories is shown in Figure 1.

Classification of adherence to commonly used medications
4.3. Factors Associated with Medication Adherence
Comparison of patients’ characteristics in terms of adherence to all four medication categories is shown in Table 2. Gender and the number of physician visits were the two characteristics not statistically associated with adherence levels to all four medication categories (all P > 0.05). For inhalant medications, all other characteristics were statistically related and associated with adherence levels (all P < 0.05). Duration of CF diagnosis, age (as a continuous variable), and body weight were the three characteristics not statistically associated with adherence levels to systemic antibiotic medications (P = 0.055, 0.064, and 0.267, respectively). In contrast, the other characteristics were related (all P < 0.05). The number of drugs, duration of CF diagnosis, mothers’ and fathers’ education, and age (as a continuous variable) were the characteristics that differed between adherence levels in gastrointestinal agents (all P < 0.05). For nutritional supplements, except for age (as a categorical variable) and the two aforementioned characteristics, all other factors varied between adherence levels (all P < 0.05).
| Medication, Associated Factors and Categories | Lower Treatment Adherence | Perfect Treatment Adherence | P-Value |
|---|---|---|---|
| Inhalants | |||
| Total | 124 (42.03) | 171 (57.97) | - |
| Gender | 0.681 | ||
| Female | 53 (42.74) | 69 (40.35) | |
| Male | 71 (57.26) | 102 (59.65) | |
| Age | 0.001 | ||
| 0.08 - 10 | 73 (58.87) | 128 (74.85) | |
| 10 - 18 | 39 (31.45) | 40 (23.39) | |
| 18 - 25 | 12 (9.68) | 3 (1.75) | |
| Number of drugs | < 0.0001 | ||
| ≤ 5 | 73 (58.87) | 149 (87.13) | |
| > 5 | 51 (41.13) | 22 (12.87) | |
| Duration of CF diagnosis (y) | 0.001 | ||
| ≤ 5 | 77 (62.10) | 137 (80.12) | |
| > 5 | 47 (37.90) | 34 (19.88) | |
| Number of physician visits | 0.056 | ||
| ≤ Twice a year | 96 (77.42) | 115 (67.25) | |
| > Twice a year | 28 (22.58) | 56 (32.75) | |
| Mother’s education levels | < 0.0001 | ||
| Illiterate | 83 (66.94) | 63 (36.84) | |
| High school diploma | 34 (27.42) | 86 (50.29) | |
| University education | 7 (5.65) | 22 (12.87) | |
| Father’s education levels | 0.002 | ||
| Illiterate | 81 (65.32) | 76 (44.44) | |
| High school diploma | 37 (29.84) | 78 (45.61) | |
| University education | 6 (4.84) | 17 (9.94) | |
| Distance to medical center | 0.001 | ||
| Tehran province | 63 (50.81) | 119 (69.59) | |
| Outside of Tehran | 61 (49.19) | 52 (30.41) | |
| Age | 8.5 (5 - 12) | 5 (1 - 10) | < 0.0001 b |
| Weight | 21.5 (14.25 - 32) | 15 (10 - 23) | < 0.0001 b |
| Systemic antibiotic | |||
| Total | 169 (67.60) | 81 (32.40) | - |
| Gender | 0.271 | ||
| Female | 75 (44.38) | 30 (37.04) | |
| Male | 94 (55.62) | 51 (62.96) | |
| Age | 0.009 | ||
| 0.08 - 10 | 101 (59.76) | 53 (65.43) | |
| 10 - 18 | 50 (29.59) | 28 (34.57) | |
| 18 - 25 | 18 (10.65) | 0 (0.00) | |
| Number of drugs | < 0.0001 | ||
| ≤ 5 | 103 (60.95) | 75 (92.59) | |
| > 5 | 66 (39.05) | 6 (7.41) | |
| Duration of CF diagnosis (y) | 0.055 | ||
| ≤ 5 | 109 (64.50) | 62 (76.54) | |
| > 5 | 60 (35.50) | 19 (23.46) | |
| Number of physician visits | 0.163 | ||
| ≤ 2 times a year | 125 (73.96) | 53 (65.43) | |
| > 2 times a year | 44 (26.04) | 28 (34.57) | |
| Mother’s education levels | < 0.0001 | ||
| Illiterate | 105 (62.13) | 25 (30.86) | |
| High school diploma | 54 (31.95) | 41 (50.62) | |
| University education | 10 (5.92) | 15 (18.52) | |
| Father’s education levels | 0.003 | ||
| Illiterate | 107 (63.31) | 33 (40.74) | |
| High school diploma | 51 (30.18) | 40 (49.38) | |
| University education | 11 (6.51) | 8 (9.88) | |
| Distance to medical center | 0.402 | ||
| Tehran province | 97 (57.40) | 51 (62.96) | |
| Outside of Tehran | 72 (42.60) | 30 (37.04) | |
| Age | 8 (5 -12) | 7 (4 - 11) | 0.064 b |
| Weight | 21 (14 - 32) | 19.5 (13 - 27) | 0.267 b |
| Gastrointestinal agents | |||
| Total | 197 (81.40) | 45 (18.60) | - |
| Gender | 0.668 | ||
| Female | 85 (43.15) | 21 (46.67) | |
| Male | 112 (56.85) | 24 (53.33) | |
| Age | 0.328 | ||
| 0.08 - 10 | 129 (65.48) | 34 (75.56) | |
| 10 - 18 | 64 (32.49) | 11 (24.44) | |
| 18 - 25 | 4 (2.03) | 0 (0.00) | |
| Number of drugs | 0.002 | ||
| ≤ 5 | 139 (70.56) | 42 (93.33) | |
| > 5 | 58 (29.44) | 3 (6.67) | |
| Duration of CF diagnosis (y) | 0.004 | ||
| ≤ 5 | 127 (64.47) | 39 (86.67) | |
| > 5 | 70 (35.53) | 6 (13.33) | |
| Number of physician visits | 0.147 | ||
| ≤ 2 times a year | 144 (73.10) | 28 (62.22) | |
| > 2 times a year | 53 (26.90) | 17 (37.78) | |
| Mother’s education levels | < 0.0001 | ||
| Illiterate | 116 (58.88) | 8 (17.78) | |
| High school diploma | 64 (32.49) | 28 (62.22) | |
| University education | 17 (8.63) | 9 (20.00) | |
| Father’s education levels | 0.010 | ||
| Illiterate | 119 (60.41) | 16 (35.56) | |
| High school diploma | 65 (32.99) | 24 (53.33) | |
| University education | 13 (6.60) | 5 (11.11) | |
| Distance to medical center | 0.093 | ||
| Tehran province | 118 (59.90) | 33 (73.33) | |
| Outside of Tehran | 79 (40.10) | 12 (26.67) | |
| Age | 8 (4 -11) | 5 (2 - 9) | 0.007 b |
| Weight | 19.8 (13.5 - 24.5) | 16 (10.5 - 27.5) | 0.106 b |
| Nutritional supplements | |||
| Total | 226 (87.94) | 31 (12.06) | - |
| Gender | 0.880 | ||
| Female | 98 (43.36) | 13 (41.94) | |
| Male | 128 (56.64) | 18 (58.06) | |
| Age | 0.068 | ||
| 0.08 - 10 | 151 (66.81) | 27 (87.10) | |
| 10 - 18 | 71 (31.42) | 4 (12.90) | |
| 18 - 25 | 4 (1.77) | 0 (0.00) | |
| Number of drugs | 0.018 | ||
| ≤ 5 | 168 (74.34) | 29 (93.55) | |
| > 5 | 58 (25.66) | 2 (6.45) | |
| Duration of CF diagnosis (y) | 0.037 | ||
| ≤ 5 | 156 (69.03) | 27 (87.10) | |
| > 5 | 70 (30.97) | 4 (12.90) | |
| Number of physician visits | 0.893 | ||
| ≤ 2 times a year | 163 (72.12) | 22 (70.97) | |
| > 2 times a year | 63 (27.88) | 9 (29.03) | |
| Mother’s education levels | 0.003 | ||
| Illiterate | 118 (52.21) | 7 (22.58) | |
| High school diploma | 88 (38.94) | 17 (54.84) | |
| University education | 20 (8.85) | 7 (22.58) | |
| Father’s education levels | 0.001 | ||
| Illiterate | 129 (57.08) | 7 (22.58) | |
| High school diploma | 82 (36.28) | 20 (64.52) | |
| University education | 15 (6.64) | 4 (12.90) | |
| Distance to medical center | 0.001 | ||
| Tehran province | 135 (59.73) | 28 (90.32) | |
| Outside of Tehran | 91 (40.27) | 3 (9.68) | |
| Age | 7 (3 -11) | 0.91 (0.67 - 5) | < 0.0001 b |
| Weight | 19 (12 - 26) | 9.8 (6.7 - 16) | < 0.0001 b |
General Characteristics of Participants in Terms of Levels of Different Medication Adherence a
Results of univariable (unadjusted) and multivariable (adjusted) logistic regression models assessing the likelihood of perfect adherence to all four medication categories are shown in Table 3. Any variables with P < 0.2 in univariable models were considered potential factors for predicting the likelihood of perfect adherence in each medication category. Age as a categorical variable was not included in all modeling processes due to estimation restrictions.
| Medication, Associated Factors and Categories | Univariable Model | Multivariable Model | ||
|---|---|---|---|---|
| Raw OR (95%CI) | P-Value | Adjusted OR (95%CI) | P-Value | |
| Inhalants | ||||
| Gender | ||||
| Female | Ref. | - | Ref. | - |
| Male | 1.10 (0.69 - 1.76) | 0.681 | - | - |
| Age | 0.91 (0.87 - 0.95) | < 0.0001 | 1.03 (0.91 - 1.17) | 0.663 |
| Number of drugs | ||||
| ≤ 5 | Ref. | - | Ref. | - |
| > 5 | 0.21 (0.12 - 0.37) | < 0.0001 | 0.32 (0.15 - 0.69) | 0.004 a |
| Duration of CF diagnosis (y) | ||||
| ≤ 5 | Ref. | - | Ref. | - |
| > 5 | 0.41 (0.24 - 0.69) | 0.001 | 0.75 (0.38 - 1.50) | 0.418 |
| Number of physician visits | ||||
| ≤ 2 times a year | Ref. | - | Ref. | - |
| > 2 times a year | 1.67 (0.98 - 2.83) | 0.057 | 1.17 (0.63 - 2.17) | 0.622 |
| Mother’s education levels | ||||
| Illiterate | Ref. | - | Ref. | - |
| High school diploma | 3.33 (1.99 - 5.58) | < 0.0001 | 2.31 (1.14 - 4.66) | 0.019 a |
| University education | 4.14 (1.66 - 10.30) | 0.002 | 2.99 (0.88 - 10.14) | 0.079 |
| Father’s education levels | ||||
| Illiterate | Ref. | - | Ref. | - |
| High school diploma | 2.25 (1.36 - 3.71) | 0.002 | 1.24 (0.62 - 2.48) | 0.540 |
| University education | 3.02 (1.13 - 8.06) | 0.027 | 1.00 (0.28 - 3.65) | 0.995 |
| Distance to medical center | ||||
| Tehran province | Ref. | - | Ref. | - |
| Outside of Tehran | 0.45 (0.28 - 0.73) | 0.001 | 0.50 (0.29 - 0.89) | 0.017 a |
| Weight | 0.96 (0.95 - 0.98) | < 0.0001 | 0.97 (0.92 - 1.03) | 0.314 |
| Systemic antibiotic | ||||
| Gender | ||||
| Female | Ref. | - | Ref. | - |
| Male | 1.36 (0.79 - 2.34) | 0.272 | - | - |
| Age | 0.94 (0.89 - 0.99) | 0.021 | 1.01 (0.87 - 1.17) | 0.914 |
| Number of drugs | ||||
| ≤ 5 | Ref. | - | Ref. | - |
| > 5 | 0.12 (0.05 - 0.30) | < 0.0001 | 0.12 (0.04 - 0.37) | < 0.0001 a |
| Duration of CF diagnosis (y) | ||||
| ≤ 5 | Ref. | - | Ref. | - |
| > 5 | 0.56 (0.30 - 1.02) | 0.057 | 0.80 (0.37 - 1.76) | 0.583 |
| Number of physician visits | ||||
| ≤ 2 times a year | Ref. | - | Ref. | - |
| > 2 times a year | 1.50 (0.85 - 2.66) | 0.164 | 0.94 (0.47 - 1.88) | 0.858 |
| Mother’s education levels | ||||
| Illiterate | Ref. | - | Ref. | - |
| High school diploma | 3.19 (1.76 - 5.79 | < 0.0001 | 2.64 (1.19 - 5.87) | 0.017 a |
| University education | 6.30 (2.53 - 15.67) | < 0.0001 | 4.23 (1.16 - 15.43) | 0.029 a |
| Father’s education levels | ||||
| Illiterate | Ref. | - | Ref. | - |
| High school diploma | 2.54 (1.44 - 4.49) | 0.001 | 1.36 (0.62 - 2.99) | 0.443 |
| University education | 2.36 (0.88 - 6.35) | 0.090 | 0.78 (0.21 - 2.92) | 0.717 |
| Distance to medical center | ||||
| Tehran province | Ref. | - | Ref. | - |
| Outside of Tehran | 0.22 (0.46 - 1.37) | 0.402 | - | - |
| Weight | 0.98 (0.96 - 1.00) | 0.091 | 1.01 (0.95 - 1.08) | 0.752 |
| Gastrointestinal Agents | ||||
| Gender | ||||
| Female | Ref. | - | Ref. | - |
| Male | 0.87 (0.45 - 1.66) | 0.668 | - | - |
| Age | 0.90 (0.83 - 0.97) | 0.009 | 0.98 (0.88 - 1.09) | 0.683 |
| Number of drugs | ||||
| ≤ 5 | Ref. | - | Ref. | - |
| > 5 | 0.17 (0.05 - 0.57) | 0.004 | 0.39 (0.1 - 1.55) | - |
| Duration of CF diagnosis (y) | ||||
| ≤ 5 | Ref. | - | Ref. | - |
| > 5 | 0.28 (0.11 - 0.69) | 0.006 | 0.36 (0.11 - 1.12) | 0.077 |
| Number of physician visits | ||||
| ≤ 2 times a year | Ref. | - | Ref. | - |
| > 2 times a year | 1.65 (0.84 - 3.26) | 0.149 | 1.16 (0.52 - 2.58) | 0.181 |
| Mother’s education levels | ||||
| Illiterate | Ref. | - | Ref. | - |
| High school diploma | 6.34 (2.73 - 14.74) | < 0.0001 | 5.95 (2.17 - 16.36) | 0.001 a |
| University education | 7.68 (2.61 - 22.60) | < 0.0001 | 8.33 (2.04 - 34.05) | 0.003 a |
| Father’s education levels | ||||
| Illiterate | Ref. | - | Ref. | - |
| High school diploma | 2.75 (1.36 - 5.54) | 0.005 | 0.93 (0.37 - 2.31) | 0.871 |
| University education | 2.86 (0.90 - 9.09) | 0.075 | 0.59 (0.14 - 2.46) | 0.473 |
| Tehran province | Ref. | - | Ref. | - |
| Distance to medical center | ||||
| Outside of Tehran | 0.54 (0.26 - 1.12) | 0.096 | 0.69 (0.30 - 1.59) | 0.385 |
| Weight | 0.98 (0.95 - 1.01) | 0.233 | - | - |
| Nutritional supplements | ||||
| Gender | ||||
| Female | Ref. | - | Ref. | - |
| Male | 1.06 (0.50 - 2.27) | 0.880 | - | - |
| Age | 0.79 (0.70 - 0.88) | < 0.0001 | 0.87 (0.63 - 1.20) | 0.393 |
| Number of drugs | ||||
| ≤ 5 | Ref. | - | Ref. | - |
| > 5 | 0.20 (0.05 - 0.86) | 0.031 | 0.71 (0.13 - 3.91) | 0.690 |
| Duration of CF diagnosis (y) | ||||
| ≤ 5 | Ref. | - | Ref. | - |
| > 5 | 0.33 (0.11 - 0.98) | 0.046 | 2.23 (0.44 - 11.27) | 0.333 |
| Number of physician visits | ||||
| ≤ 2 times a year | Ref. | - | Ref. | - |
| > 2 times a year | 1.06 (0.46 - 2.42) | 0.893 | - | - |
| Mother’s education levels | ||||
| Illiterate | Ref. | - | Ref. | - |
| High school diploma | 3.26 (1.29 - 8.19) | 0.012 | 1.15 (0.36 - 3.71) | 0.817 |
| University education | 5.90 (1.87 - 18.63) | 0.002 | 3.67 (0.79 - 17.02) | 0.096 |
| Father’s education levels | ||||
| Illiterate | Ref. | - | Ref. | - |
| High school diploma | 4.49 (1.82 - 11.10) | 0.001 | 2.79 (0.89 - 8.79) | 0.079 |
| University education | 4.91 (1.29 - 18.76) | 0.020 | 2.58 (0.48 - 14.03) | 0.271 |
| Distance to medical center | ||||
| Tehran province | Ref. | - | Ref. | - |
| Outside of Tehran | 0.16 (0.05 - 0.54) | 0.003 | 0.19 (0.05 - 0.73) | 0.015 a |
| Weight | 0.91 (0.86 - 0.96) | < 0.0001 | 0.94 (0.83 - 1.08) | 0.406 |
Results of Logistic Regression Modeling for Associated Factors of Different Medication Adherence
4.4. Inhalants
All factors were entered into the multivariable model except for gender (P > 0.2) for inhalants. Among the other factors entered, only the number of drugs, the mother’s education, and distance to the medical center were statistically significant predictors of perfect adherence, controlling for all other factors in the model. Taking more than 5 drugs per day compared to 5 or fewer drugs decreased the likelihood of perfect adherence by approximately 68% (odds ratio [OR], 0.32; 95% CI, 0.15 - 0.69; P = 0.004). High school education of patients’ mothers increased the likelihood of perfect adherence more than twofold compared with mothers who were illiterate (OR, 2.31; 95% CI, 1.14 - 4.66; P = 0.019), and university education of patients’ mothers approximately tripled the likelihood of perfect adherence compared to illiterate mothers (OR, 2.99; 95% CI, 0.88 - 10.14; P = 0.079). Living outside Tehran province also reduced the likelihood of perfect adherence by up to 50% (OR, 0.50; 95% CI, 0.29 - 0.89; P = 0.017).
4.5. Systemic Antibiotics
In the context of systemic antibiotic medication, only the number of drugs and a mother’s education among the seven potential factors were statistically significant predictors of perfect adherence. Taking more than 5 drugs per day compared to 5 or fewer drugs reduced the likelihood of perfect adherence by approximately 88% (OR, 0.12; 95% CI, 0.15 - 0.69; P < 0.0001). Compared with mothers who were illiterate, mothers with a high school education increased the likelihood of perfect adherence by more than two and a half times (OR, 2.64; 95% CI, 1.19 - 5.87; P = 0.017), and mothers with a university education improved the likelihood of perfect adherence by more than four times (OR, 4.23; 95% CI, 1.16 - 15.43; P = 0.029).
4.6. Gastrointestinal Agents
In the context of gastrointestinal agents, the mother's education is the only robust, statistically significant predictor of perfect adherence. Compared to mothers who were illiterate, mothers with a high school education significantly increased the likelihood of perfect adherence (OR, 5.95; 95% CI, 2.17 - 16.36; P = 0.001), and mothers with a university education further improved the likelihood of perfect adherence (OR, 8.33; 95% CI, 2.04 - 34.05; P = 0.003).
4.7. Nutritional Supplements
Distance to the medical center is the only statistically significant predictor of perfect adherence to dietary supplements and medications. Results of the adjusted model indicate that living outside of Tehran decreases the likelihood of perfect adherence by up to 81% (OR, 0.19; 95% CI, 0.05 - 0.73; P = 0.015).
5. Discussion
Medication adherence in CF, a lifelong disease with complex, costly, and time-consuming treatment, is crucial. To the best of our knowledge, this is the first study to evaluate medication adherence and associated factors in Iranian patients with CF. Our findings showed low adherence to commonly used medications in approximately 87% of children and adolescent patients with CF. A targeted literature review by Narayanan et al. assessed 19 published studies from 2010 to 2016 on adherence rates to different CF treatments and demonstrated that adherence to CF therapies is moderate-to-low (suboptimal) and varies significantly by treatment type, mode of treatment administration, method of adherence measurement, and also by age, season, and time (17). Later studies also confirm the findings of low adherence to medical treatment in CF patients (18, 19).
Among the commonly used medication classes in CF, inhalants, the most used medications in studied patients (in more than 98%), had the highest adherence rate (~ 58% with perfect adherence). In contrast, nutritional supplements had the lowest adherence (~ 12% with perfect adherence). Higher adherence to respiratory tract medications (i.e., inhalants and systemic antibiotics) in studied patients may be explained by the fact that pulmonologists run the CF Clinic in Iran, and CF is also known as a lung disease to most people. Therefore, patients and their parents may be more likely to adhere to medications targeting the lung. Studies on pancreatic enzyme replacement therapy or vitamins also showed much lower adherence levels than some inhaled therapies and antibiotics (6, 20, 21). It should be noted that among patients with CF, adherence to one class of medication cannot predict adherence to other medication classes, as reported by similar studies.
This study found that perfect medication adherence in children with CF was associated with the number of drugs, the mother’s education level, and distance from the medical center. Specifically, taking more than five drugs per day decreases the likelihood of perfect adherence to inhalants and systemic antibiotics. The high school and university education level of patients’ mothers increases the likelihood of perfect adherence compared with illiterate mothers for inhalants, systemic antibiotics, and gastrointestinal agents. Living outside of Tehran province decreases the likelihood of perfect adherence to inhalants and nutritional supplements. A high level of polypharmacy (i.e., an increased number of treatments taken each day) is identified as a barrier to adherence (5, 6). However, similar to our results, Zindani et al. did not find a significant correlation between the total number of medications and adherence to dornase alfa or multivitamins in CF patients (11). Mothers' university education positively affected adherence to inhalants, systemic antibiotics, and gastrointestinal agents. Previous studies have shown that children of parents with lower educational attainment are less adherent to medications for chronic diseases like attention deficit hyperactivity disorder (ADHD), glaucoma, and transplant (22-24). Besides the psychological status of the parents, the level of stress of the patient and parents is involved in medication adherence (25). Management of parent behaviors, such as parent training, is known to promote adherence among chronically ill youth (26). Therefore, future research on improving a mother’s knowledge may be crucial for better medication adherence in pediatric patients with CF. Living far from the medical center was another predictor of adherence for inhalants and nutritional supplements. In a study evaluating the effects of distance traveled on adherence to treatment, families who lived more than 20 miles from a pediatric dermatology clinic were more likely to be non-adherent to the treatment plan (27). This highlights the need to increase the number of pediatric medical centers across the country, particularly in underserved areas.
The researchers observed no significant correlation between adherence to commonly used medications and the patient’s gender, age, body weight, father’s education level, number of physician visits, and disease duration. Various studies investigating barriers influencing adherence to CF therapies have yielded contradictory results. Although several previous studies have demonstrated that treatment adherence decreases with advancing age, disease severity, and long disease duration, others found no significant relationship (12, 18, 20, 21, 28, 29).
Several direct and indirect methods have been used to determine patients’ medication adherence in CF. Among them, the Medication Adherence Rating Scale (MARS) describes an individual's medication adherence by evaluating attitudes about medications and actual medication-taking behavior (30). Using the MARS-5 questionnaire in this study as an objective measurement tool appears to be a more reliable and valid method for estimating compliance — rather than using self-report methods — by having the researcher read and explain the questions to the patients and parents.
5.1. Study Limitations
The major limitation of the present study is the lack of evaluation of the impact of adherence rates on clinical outcomes. The relationship between low adherence to medication and clinical variables with larger sample sizes from multicenter studies is needed to elucidate the complex relationships between adherence to treatment and various aspects of CF management. Moreover, additional factors such as parental age and the socioeconomic status of patients can be considered as influencing factors of medication adherence in future studies.
5.2. Conclusions
Non-adherence to inhalants, systemic antibiotics, gastrointestinal agents, and nutritional supplements is common in children and adolescents with CF, and adherence to one class of medication cannot predict adherence to others. Taking more than five drugs is associated with lower adherence to inhalants and systemic antibiotics. Additionally, living far from the medical center is related to lower adherence to inhalants and nutritional supplements. Conversely, a high education level of patients’ mothers increases the likelihood of perfect adherence to inhalants, systemic antibiotics, and gastrointestinal agents. Educational interventions with planned patient monitoring may be needed to improve medication adherence in the pediatric CF population.
