SARS-CoV-2 is a positive single-strand RNA virus from the Coronaviridae family, which has become a global pandemic. The disease known as COVID-19 is highly contagious and has become a significant health burden due to its widespread and varied mechanisms of pathogenesis. The cardiovascular system can be affected by the virus (
2).
Atherosclerosis is a severe and chronic inflammatory disease characterized by thickened artery walls. This increased thickness and plaque accumulation lead to narrowed and tightened channels, raising blood pressure. Several factors contribute to the development of this disease, including high cholesterol, hypertension, hyperglycemia, and smoking. Recently, some viral infections have also been reported to contribute to the disease's development (
18). Atherosclerosis may provide suitable conditions for SARS-CoV-2 viral propagation, and conversely, COVID-19 can influence atherosclerosis development by inducing plasmatic cytokines and inflammatory pathways. A meta-analysis revealed a higher incidence of hypertension and cardiovascular disease in severe cases among 53,000 COVID-19 patients (
19). In this study, parameters related to fat metabolism such as triglycerides, LDL, and HDL; inflammatory pathways such as LDH; the renin-angiotensin system including ACE and ACE2; and the susceptibility of COVID-19 patients to atherosclerosis were examined as described previously.
Lipid metabolism could be affected in COVID-19 patients (
20). Although only cholesterol levels among the lipid profiles in our study significantly differed between severe and non-severe cases, decreased HDL levels and increased total cholesterol, LDL, and triglyceride levels were observed with disease severity. Previous studies have reported reductions in total cholesterol and HDL in COVID-19 patients, but triglyceride levels and the cholesterol to HDL ratio were higher in those patients (
20). A study by Wang et al. (
21) reported the effect of higher tissue cholesterol content on COVID-19 severity due to vascular inflammation associated with tissue macrophages overloaded with cholesterol.
Low-density lipoprotein is the main lipoprotein accumulating in the sub-endothelial space and causes arterial wall inflammation after oxidation. TLR4/NFkB and JAK/STAT are inflammatory pathways involved in atherosclerosis, leading to induced inflammation, cytokine expression, and activation of the innate and adaptive immune systems (
22,
23). High cholesterol levels trigger a pro-inflammatory state and increase patients' susceptibility to both COVID-19 and atherosclerosis.
As mentioned, the total cholesterol to HDL ratio is a good marker for the risk of cardiovascular diseases and atherosclerosis. The study results showed no significant difference in the chol/HDL ratio among patients with severe and non-severe COVID-19, but this difference was highly significant between the patients and the control group. The mean chol/HDL ratio was about 4 in both patient groups and 2.5 in healthy cases. Since ratio values above 3.5 are considered high risk for cardiovascular diseases (
12), it can be concluded that COVID-19 increases the vulnerability to cardiovascular diseases and atherosclerosis.
TNF-α is an inducer for HDL and cholesterol levels. A previous study has shown that blocking TNF-α leads to an increase in total cholesterol and HDL levels (
24). High-density lipoprotein has also been reported to decrease TNF-α levels by downregulating TLR-2, which is responsible for TNF-α production (
25). IL-1 can induce IL-6, TNF-α, IL-8, and chemokines. CD14++ and CD16+, which are atherosclerosis-dependent monocytes, can also induce IL-1, TNF-α, and IL-6 (
3). Increased levels of cytokines and switched immune cells are observed as inflammatory agents in both atherosclerosis and severe COVID-19 patients (
26,
27). The current study showed an increase in total cholesterol levels in severe cases, but the HDL level was found to be decreased in those patients. Thus, TNF-α and IL-1 could be proper candidates for further investigations to find out the mechanism behind the changes in the lipid profile of the patients.
The importance of IL-1, IL-6, and TNF-α also makes them appropriate targets for therapies of inflammatory states in coronary heart disease and COVID-19 (
3). Some commercial monoclonal antibodies have already been developed, including Canakinumab (IL-1b mAb) (
28), Anakinra (IL-1R antagonist) (
29), tocilizumab (IL-6R mAb) (
30), and some anti-TNF antibodies which increase HDL levels for rheumatoid arthritis treatment including Etanercept, infliximab, and adalimumab (
31-
34). Low-dose colchicine treatment, which disrupts inflammasome activation, has also been proposed for controlling cardiovascular problems in patients with chronic coronary disease (
35).
During COVID-19, the pro-inflammatory cytokines lead to oxidative stress due to the generation of free oxygen and halogen-containing radicals by endothelial and blood cells, which could develop atherosclerosis. These could lead to LDL oxidation, making it a neoantigen and leading to autoimmune processes in plaques (
36).
Numerous studies at the pandemic's beginning reported cardiac injury in one-third of COVID-19 patients with increased levels of cardiac biomarkers such as troponin (
37). SARS-CoV-2 infection induces many cytokines that can trigger a cytokine storm and atherosclerosis (
2,
3). COVID-19 patients also show ST-segment elevation during electrocardiography, myocardial infarction, and acute myocarditis with very high levels of troponin (
38,
39). Consistent with these results, our study showed a significant increase in troponin levels with disease severity, which implies the effect of COVID-19 infection on cardiac complications, including atherosclerosis.
CD147 is a glycoprotein from the immunoglobulin superfamily and acts as a SARS-CoV-2 receptor beside conventional ACE2. In our study, CD147 was similarly increased with disease severity, and its level was significantly higher in severe cases compared to non-severe. CD147 can induce inflammatory factors through the NF-kB pathway, and it has been reported to be upregulated in various inflammatory diseases (
40).
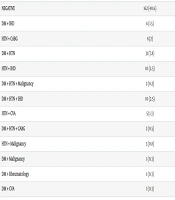
In accordance with the results of this study, further investigations clarified that patients with normal levels of CD147, ACE, troponin, LDH, LDL, triglycerides, and cholesterol were less likely to experience severe disease and had a lower chance of being admitted to the ICU. Since CD147, ACE, and cholesterol were the distinct parameters with significant differences between severe and non-severe cases and also showed higher risk for disease severity in non-normal levels, they can be considered candidate biomarkers of COVID-19 severity. Among the mentioned parameters, only ACE and CPKmb levels were statistically significant risk factors.
MAPK and JAK/STAT are other signaling pathways that CD147 employs in pathological processes (
40). Coronary artery disease also presents overexpression of CD147 in platelets, monocytes, granulocytes, and soluble forms (
41). Low-density lipoproteins, CRP, advanced glycation end products, and high glucose are factors that can upregulate CD147 in inflammatory cells (
42-
44). CD147 is overexpressed in plaques and accumulates around macrophages, SMCs, and MMP-9-positive cells (
45,
46). CD147 induces angiogenesis, and experiments have reported that inhibiting it with siRNA diminishes angiogenesis (
47). In this study, the increased amounts of CD147 in severe COVID-19 cases also represent the higher risk for atherosclerosis development.
ACE2 on the surface of epithelial cells is the substantial receptor for SARS-CoV-2 (
18). Both ACE and ACE2 are included in the renin-angiotensin system. In the present study, both ACE and ACE2 levels increased with disease severity, but only ACE was significantly different in comparison to severe and non-severe cases. The difference between the ICU (severe) and non-severe groups was not significant for ACE2, whereas the significant difference was between severe and non-severe groups compared to control groups. ACE2 has been reported to be upregulated in severe COVID-19 patients, and its increase is highly correlated with cardiovascular diseases (
48-
50). These observed differences include both soluble and cell-attached forms of ACE2. The ACE2/ACE ratio was previously reported to have decreased in most chronic diseases (
51).
Angiotensin-converting enzyme 2 mediates the degradation of Ang II to Ang 1 - 7 and Ang I to Ang 1 - 9. Ang 1 - 7 plays anti-inflammatory roles, while ACE modulates inflammation. Viral replication downregulates ACE2 during virus entry into the host cell. Ang II leads to vast adverse effects, including myocardial hypertrophy, intestinal fibrosis, endothelial injury, increased inflammation, hypertension, oxidative stress, and higher levels of coagulation. It also activates the immune system, including macrophages, by inducing IL-6, TNF-α, and other inflammatory cytokines (
52,
53). Thus, increasing soluble and membrane-attached ACE2 plays protective roles against COVID-19 (
54).
A cholesterol-rich region in the membrane of host cells is related to virus attachment to the ACE2 receptor. In a study of cardiovascular patients, NLRP3 inflammasome is activated by intracellular cholesterol in macrophages, aiding the progression of both the COVID-19 cytokine storm and atherosclerosis. The scavenger class B receptor type 1 (SR-B1) is a cholesterol receptor protein that binds to HDL and interacts with the S1 subunit of the spike protein, facilitating better viral infection spread (
55). Thus, cholesterol, HDL, and ACE2 work together in disease progression, cytokine storm, and the potential development of coronary artery disease. In this study, ACE2 was found to be correlated with both cholesterol and HDL.
Lactate dehydrogenase is a cytoplasmic enzyme present in various tissues, and its levels may increase in malignancies, lung disease, tissue injury, hypoxia, necrosis, myocardial ischemia, and hemolysis (
56). Lactate dehydrogenase levels over 557 have been reported to be positively correlated with in-hospital mortality of cardiovascular patients (
57). Both LDH and CRP have been reported to correlate with COVID-19 severity and have been proposed as predictors of respiratory failure in COVID-19 patients (
58,
59), consistent with the results of this study. Lactate dehydrogenase also increased with disease severity in this study, which can be a triggering factor for developing atherosclerosis.
Our study shows that CPK and CPKmb levels were highest in non-severe patients in the ward, followed by ICU patients, and lowest in healthy cases. One study reported that CPK and CPKmb levels increased due to atherosclerosis and endothelial dysfunction (
60). On the other hand, resveratrol, an atherosclerosis drug, inhibits the PI3K/AKT/mTOR pathway, leading to decreased CPK levels (
60). Therefore, higher CPK and CPKmb levels in the patient (severe and non-severe) groups could represent a hypothetical maximum level that leads to the worst disease condition.
The results showed that CD147 correlated with troponin. CD147 and ACE2 contribute to virus infection by binding to the spike protein, and a strong correlation was found between them in this study. Thus, a hypothetical ratio of ACE2/CD147 was assessed among the studied groups. This ratio was significantly correlated with troponin. Since troponin is a cardiac biomarker and due to the intrinsic roles of ACE2 and CD147 in COVID-19 disease, the correlation of troponin with the ACE2/CD147 ratio can effectively link COVID-19 with atherosclerosis.
5.1. Conclusions
The results also showed that normal levels of CD147, ACE, Troponin, LDH, LDL, Triglyceride, and Cholesterol are associated with lower COVID-19 severity. Among these candidate biomarkers for COVID-19 severity, CD147, ACE, Troponin, and Cholesterol levels are the most promising due to their significant difference between severe and non-severe cases.
According to the present study on the relationship between atherosclerosis and COVID-19, and based on the results of recent studies, ACE and CD147 can be considered vital serum biomarkers in diagnosing atherosclerosis susceptibility in these patients. They may also serve as useful tools for monitoring and preventing the progression of atherosclerosis. This study suggests that CD147 and ACE levels could be potential biomarkers for assessing susceptibility to atherosclerosis among COVID-19 patients. Further investigations are recommended to confirm these findings. Our work should address limitations such as the small sample size and the examination of other inflammatory factors.
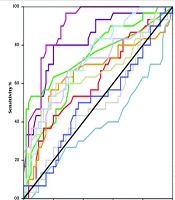








 analysis of the studied parameters. The results proposed angiotensin-converting enzyme (ACE) and CD147 as the best biomarkers for the susceptibility of COVID patients to atherosclerosis.")