Acetaminophen is a widely used analgesic and antipyretic which is available over the counter. Lack of gastrointestinal side effects and rapid absorption has made it a popular analgesic in the last four decades. As hepatotoxicity is a common complication following acetaminophen overdose, it can terminate acute liver failure (ALF). One of the most common causes of ALF in both the USA and UK is Acetaminophen (
1). Nowadays, without treatment, acetaminophen overdose leads to 0.4% mortality, and in at least half of people with blood level acetaminophen above the UK standard treatment line manifests with severe liver damage (
2). Cerebral edema is a major cause of death in acute acetaminophen overdose (
3). Acetaminophen poisoning accounts for at least 42% of USA acute liver failure cases seen at tertiary-care centers and one-third of the death. The number of ALF cases due to acetaminophen poisoning doubled within six years (
4). in recent years, the proportion of admissions involving acetaminophen increased significantly in the UK (
5,
6). Another study in Canada showed that the incidence of acetaminophen overdose was 46 per 100,000 populations in the last decade (
7,
8). Generation of reactive oxygen species and nitric oxide, lipid peroxidation, mitochondrial dysfunction, disruption of calcium hemostasis, and induction of apoptosis are all mechanisms suggested may be involved in acetaminophen-induced hepatotoxicity (
3,
9). Numerous biomarkers for drug-induced liver injury have been explored, but less than ten are adopted or qualified as valid by the US FDA (Food and Drug Administration) (
10). Increase in plasma activities of aspartate aminotransferase (AST) and alanine aminotransferase (ALT) (
11,
12), glutathione peroxidase (GPx) (
13,
14), lactic dehydrogenase (LDH) and hydroxybutyrate dehydrogenase (HBDH) (
15,
16), glutathione S-transferase (GST) (
17), argininosuccinate synthetase (
18), Pentraxin 3 (
19), F-protein (
20), bilirubin (
21), blood ammonia concentrations (
22), hypoglycemia (
23), prolongation of prothrombin time (PT) (
24) or international normalized ratio (INR) (
25,
26), and early high anion gap metabolic acidosis (
27) have already been introduced as biomarkers of acetaminophen-induced liver damage. Arginase I, sorbitol dehydrogenase (SDH), ornithine carbamyltransferase (OCT), glutamate dehydrogenase, paraoxonase, malate dehydrogenase, and purine nucleoside phosphorylase have also been introduced as biomarkers of liver necrosis (
28). All the biomarkers as mentioned above are usually obtainable 48 h following acetaminophen overdose. Taurine (2-aminoethane sulfonic acid) is a β-amino acid being of a sulfonic acid group substituted instead of a carboxylic acid group in the standard proteinogenic amino acids’ structures. The mammalians brain, heart, liver, neutrophils, retina, and kidneys contain high concentrations of taurine, a conditionally essential amino acid which is one of the most abundant free amino acids that is not included in protein structure (
29). taurine plasma and urine concentrations vary following surgical trauma (
30), muscle necrosis, stress stages, e.g. osmotic changes, anoxia, cell proliferation, brain development (
31), stroke, speedy exercise (
32), hepatic encephalopathy (
33), and heroin addiction (
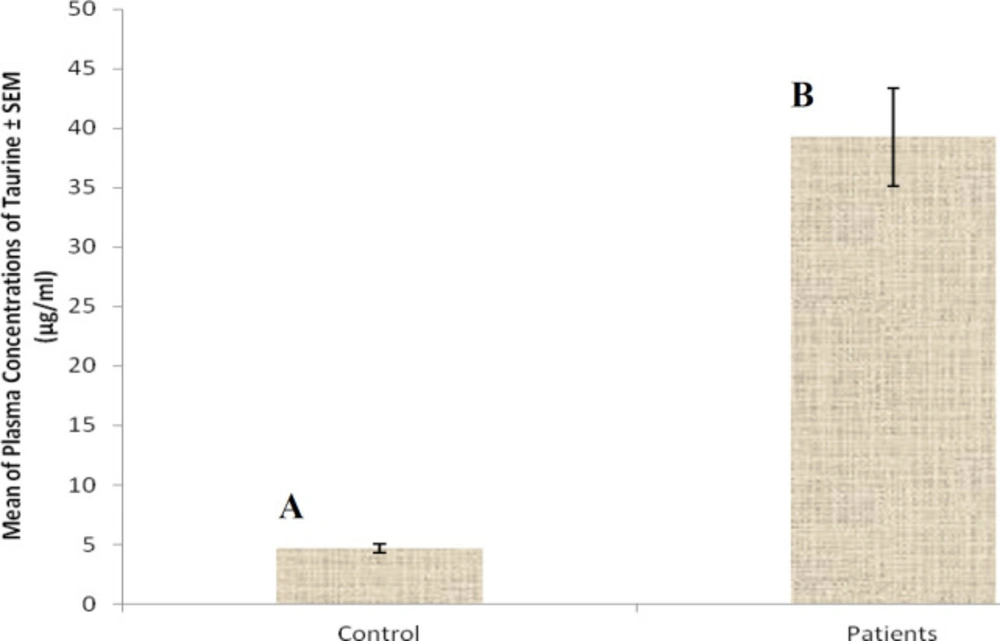
34). Our study determined that mean plasma taurine level (26.4 ± 1.6 mg/L) in acetaminophen-overdose patients was significantly greater comparing to healthy humans (5.6 ± 0.2 mg/L) (
P < 0.0001) (
35). In our previous study, we were not able to show frequency of changes in plasma concentration of taurine during poisoning. Therefore, the aim of this study was to follow up those changes during the three days period following acetaminophen overdose.