Although several trials and meta-analyses have previously examined the effect of a high protein diet in ICU patients (
19). This study is the second RCT that examined the effect of a high protein diet in neurocritical patients. In this randomized clinical trial, we evaluate the impact of a high protein diet on the nutritional biomarker (nitrogen balance and serum level of TTR) and clinical status in neurocritical patients. The sample groups matched concerning demographic and clinical characteristics such as age, sex, BMI, APACHE II score and baseline of GCS, ICH score, SAH grading, and the Marshall score of TBI patients. Our findings revealed that the 28-day mortality rate was significantly lower in the intervention group. We observed a significant relationship between the higher APACHE II score, lower the baseline serum level of TTR, a negative baseline nitrogen balance, and older age with the lower GOSE outcome. Therefore, we came to that conclusion: a high protein regime may have a significant role in improving the GOSE outcome, and decreasing mortality rate because of a significant difference was observed in the nitrogen balance on the fifth day and three months GOSE clinical outcomes between both groups, and the baseline serum level of TTR, NB, age, and APACHE-II score are the prognostic factors for predicting GOSE outcome. APACHE II score is one of the most specific prognostic factors for ICU patient. This standard score is useful for predicting the mortality rate in the ICU patients with a different diagnosis (
21). Also, we used this score to compare the severity of the disease and mortality rate in our patients with a different mechanism of brain injury. Since, due to the nonsignificant difference of this score between the two groups, we can ignore the variation in the mechanism of brain injury that was considered as a confounding factor. In a recent study, the results showed the performance of the APACHE-II score was higher discrimination than the ICH score (
22). Currently, available evidence on the good functioning of APACHE-II in the neurocritical patient is available (
26,
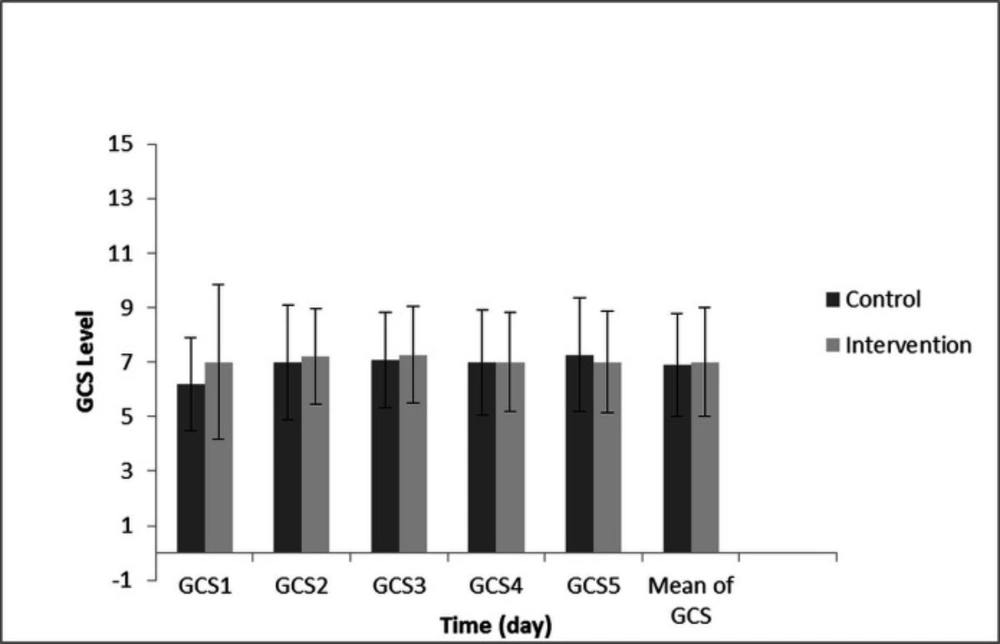
27). The initiate GCS has become a fundamental aspect of the clinical care of the patients with TBI (GCS), aneurysmal SAH (HuntHess and WFNS), ICH patients (ICH score) and ischemic stroke (NIHSS) (
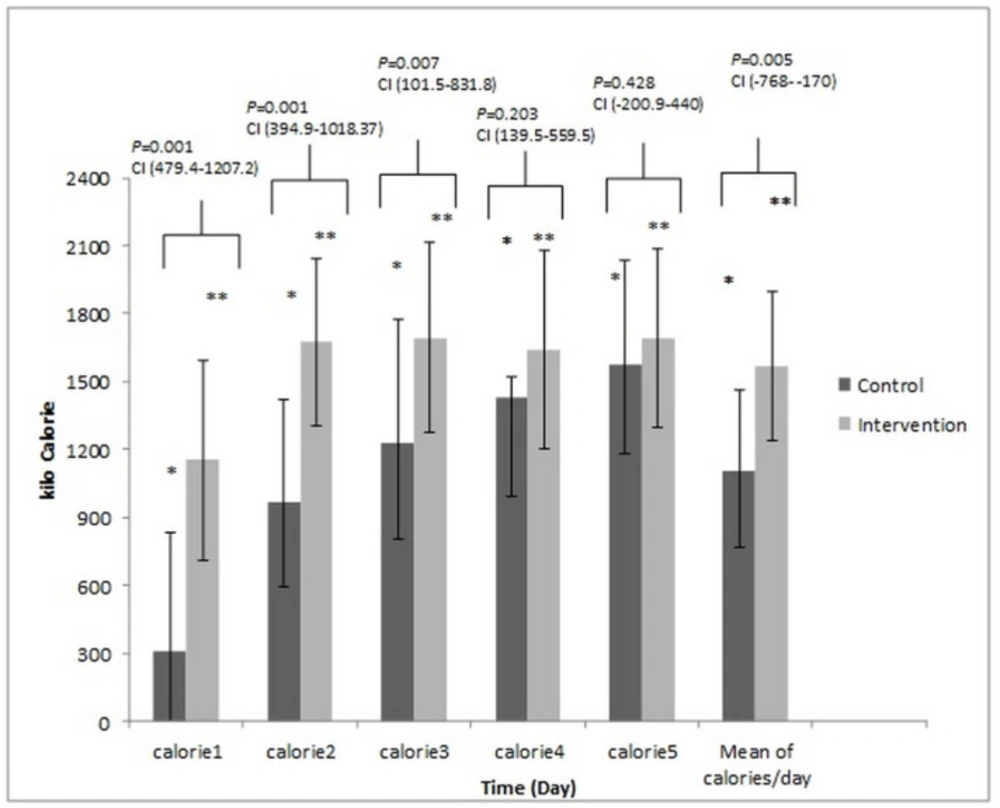
22). Therefore, in our study, the initiate GCS of the patients was recorded and used for standardized assessment of all of the patients. Also, to further evaluate the severity of the disease in each patient category; ICH score, SAH grading, the Marshall score of TBI patients, size and location of tumors recorded that there was no difference between the two groups. Malnutrition can cause multi-organ failure, more infection, and prolonged mechanical ventilation dependency. A higher protein diet can reduce these complications and a better clinical outcome (
19). Similarly, the 28-day mortality rate is significantly lower in the intervention group in our study. Similar to our findings, previous studies indicated age, and the APACHE-II score is the prognostic factors about the clinical outcome (
28). In a clinical trial 118 ICU patients were examined, the result showed that the serum level of TTR on the third and seventh days of ICU admission did not increase, although the patients received enough calories and protein intake (
29). Similar to the results of our study, the serum levels of TTR did not have a significant difference on different days in two groups and intragroup. In a clinical trial, the results showed that the patients with the lower baseline serum TTR before surgery had the longest stay in the hospital and ICU. Also, they had higher mortality and infection rates (
15). Until 2018, only two studies examined the effect of a high protein diet on the clinical outcome in neurocritical patients, and only four clinical trials examined the effect of a high protein diet on the medical or surgical adult ICU patients (
19). In the first study, Clifton
et al., 20 head trauma patients were studied in two different groups. But there was no difference in the mortality rate and clinical outcome. But the results of our study were contrary to this study. This may be due to the following reasons; in the Clifton study, the control group received 14%, and the intervention group, 22% of its calories as protein but in our study protein was not used to provide calories. Also, in the Clifton study, the mean of nitrogen balance during seven days of the study was negative in both groups, but in our study, the mean of nitrogen balance of intervention group became positive (
30). In the Second study, Oertel
et al. reported that the GOS scores were higher when neuro ICU patients received a protein-rich diet (
11). Also, the result of the different studies showed the TTR serum level was the predicting factor for the clinical outcome, and mortality after surgery, in TBI and stroke patient. In a clinical trial, 117 ischemic stroke patients were examined, and the results showed that the patients who had lower serum levels of TTR, had a lower GOSE outcome (
31). In another study, 81 ischemic stroke patients were examined, and the results showed the baseline serum level of TTR was an important predicting factor for the one-year mortality and clinical outcome (
32). The similar results were reported in different studies. Also, in different studies, the results showed the baseline serum level of TTR had a direct relationship with an Injury Severity Score (ISS), and an APACHE-II score and higher ISS or APACHE-II is associated with lower TTR levels. Similar results were obtained from our study (
16-
18). Jivnani
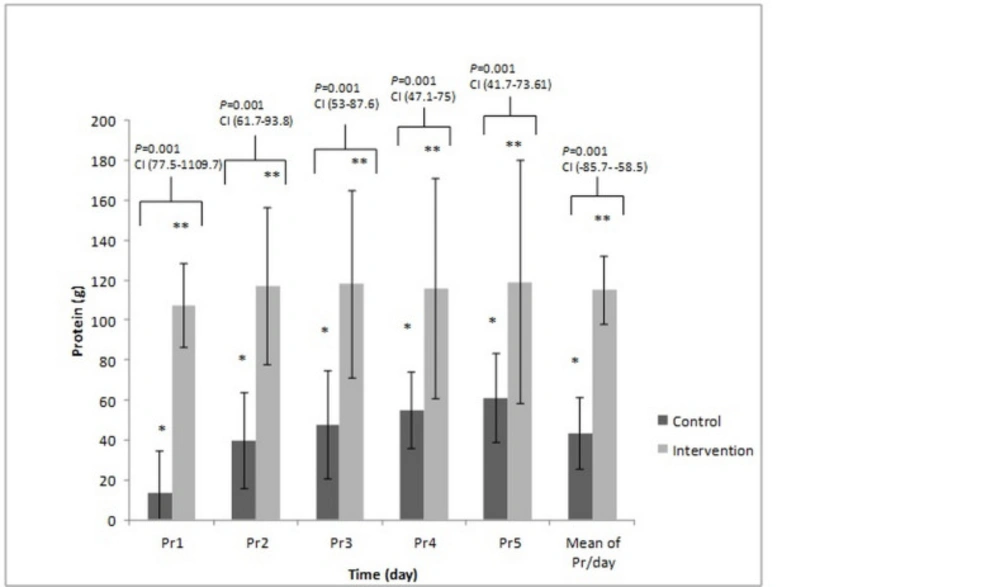
et al. reported the hypercatabolic state after brain injury can cause a negative nitrogen balance and rapidly start of central feeding can cause an increase in nitrogen balance and better clinical outcome (
17). Nataloni
et al. also, reported a direct relationship between nitrogen balance and the severity of the injury. Other studies demonstrated that a negative nitrogen balance had a significant association with the worsened clinical outcome (
18). A similar result was found in our study. In this randomized clinical trial, we evaluated the effects of a high protein diet on the nutritional biomarkers and clinical status in neurocritical patients, and a significant difference was observed in the nitrogen balance on the fifth day, three-month GOSE clinical outcome and mortality rate between both groups. Unfortunately, the different prognosis of various diseases is a confounding factor in our study and can affect the significance of the result. Although the APACHE II score is intended to evaluate the uniformity of severity of injury between the two groups, and there was no significant difference between the two groups. Also, the severity of the disease in each patient category; ICH score, SAH grading, the Marshall score of TBI patients, size and location of tumors evaluated, and there was no significant difference between the two groups. Because of the limited sample size that was related to the single-center study, and a long period to complete this sample size, we believe that the findings provide an additional benchmark for further studies involving more patients and longer duration of intervention.