Twenty-one patients were treated with insulin as protocol A and 23 of them were introduced to protocol B (metformin treatment). Mean age of insulin and metformin-treated patients was 50 ± 21.68 and 48.4 ± 16.77 respectively.
Initial experimental evaluations and clinical assessments weretaken from patients of two groups in the admission period (
Table 1).
| Protocol A: Insulin treatment group | Protocol B: Metformin treatment group | p-value |
|---|
| Age | 50 ± 21.68 | 48.4 ± 16.77 | |
| BS (mg/dL) | 149.25 ± 10.31 | 177.81 ± 20.17 | 0.32 |
| MAP (mmHg) | 94.7 ± 12.15 | 86.9 ± 7.14 | 0.07 |
| HCO3 (mEq/L) | 23.15 ± 2.30 | 23.80 ± 3.54 | 0.69 |
| pH | 7.42 ± 0.05 | 7.37 ± 0.11 | 0.15 |
| APACHE II | 23.25 ± 6.92 | 20 ± 6.32 | 0.42 |
| G.C.S | 9.5 ± 3.93 | 7.4 ± 3.78 | 0.20 |
There was no significant difference between thefirst BS levelof theadmitted patients forthe two different protocols (p = 0.32). Moreover, mean arterial pressure (MAP), serum HCO
3 and pH levels were not statistically significant betweenthe patients of two groups in admission (p= 0.07, 0.69 and 0.15 respectively,
Table 1). In addition, APACHE II and G.C.S have not showed significant difference for admitted patients of both groups in first day before the treatment.
BS: Blood Sugar; MAP: Mean Arterial Pressure; APACHE II: Acute Physiological and Chronic Health Evaluation; G.C.S: Glasgow Coma Scale.
Blood sugar monitoring for three days of treatment
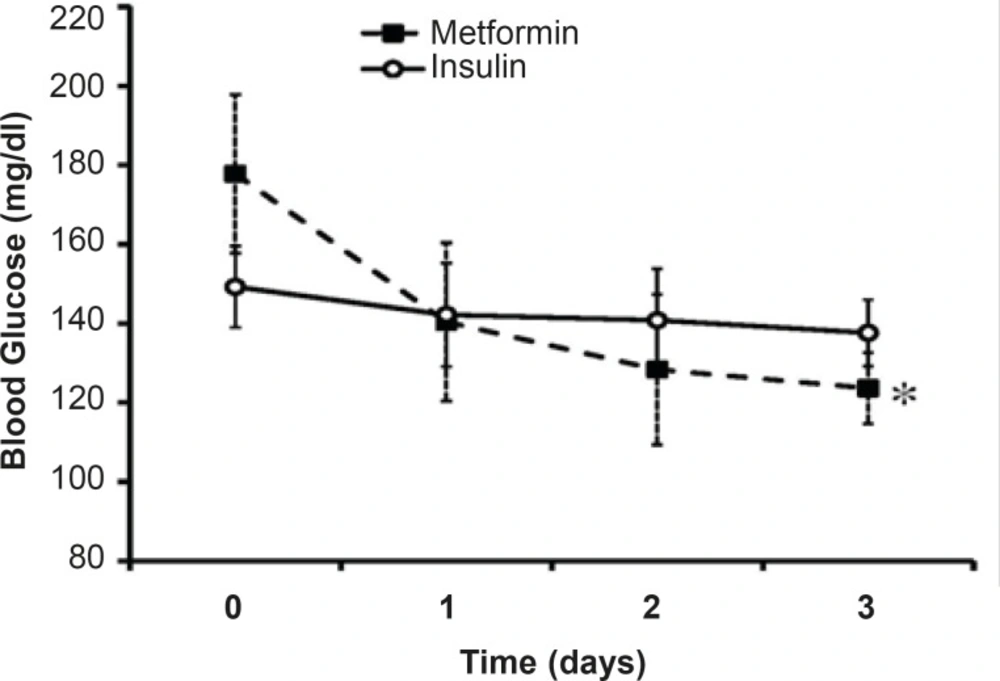
The mean levels of BS along three days of treatment were 140.19 ± 6.32 mg/dL in insulin-treated group and 130.77 ± 2.1 mg/dL in metformin-treated group. Although the mean level of BS in metformin-treated group was less thanthat of the other group, the difference was not significant (
Figure 1). In insulin-treated group, the men’s level of BS in the 1
st day of admission was 149 mg/dL that reached to 137.61 mg/dLin the 3
rd day of insulin treatment (p=15). Metformin reduced BS from 177 mg/dL in the1
st day of admission to 123.63 mg/dL in the 3
rd day of treatment (p <0.01;
Figure 1).
Effects of intensive insulin-therapy or metformin oral administration on blood sugar levels.Day 0 shows the BS levels before the beginning of each protocol. Data were expressed as mean ± SEM. *: p < 0.01 in comparison with BS levels obtained before the onset of metformin treatment
Desirable BS level (80 mg/dL<BS< 120 mg/dL) was not achievedthrough three days of insulin treatment (137.61 mg/dL) whileit reached near the normal range after three days of metformin treatment (123.63 mg/dL).
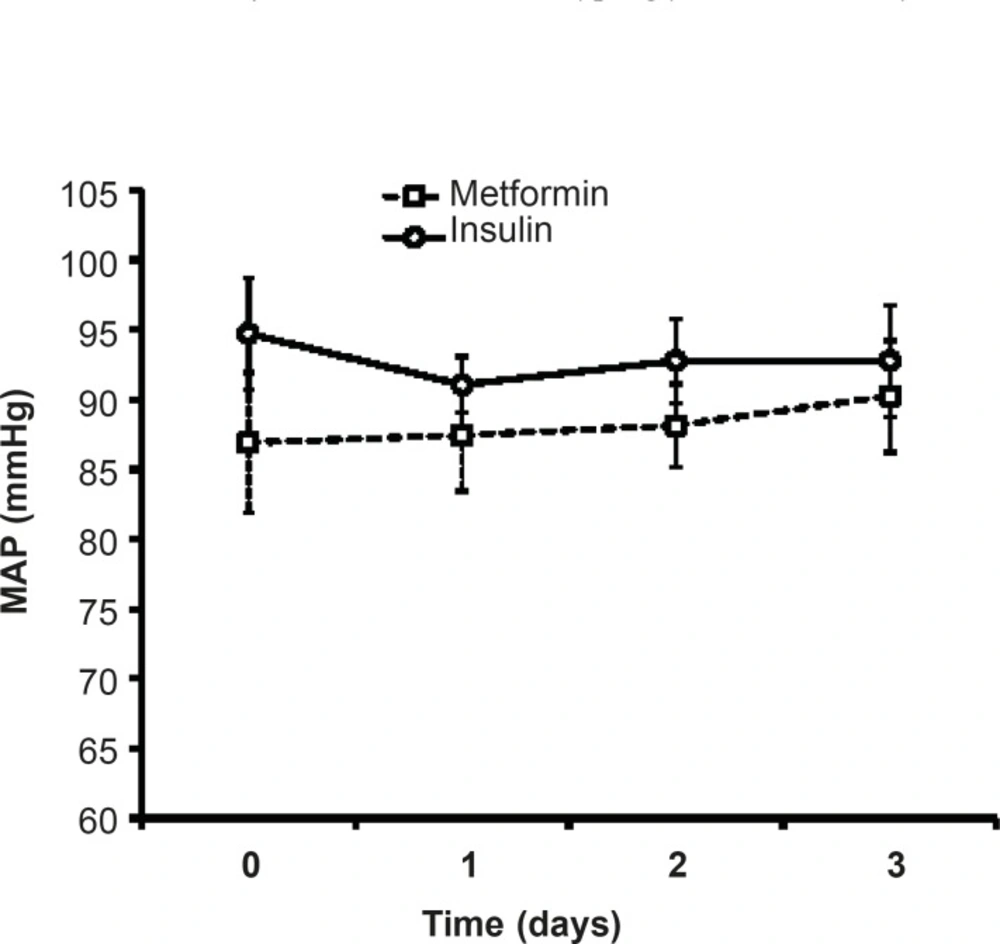
Effects of different protocols on MAP
As shown in
Figure 3, there was no significant difference in MAP of patients treated with insulin compared to metformin-treated patients.During three days of insulin or metformin treatment, MAP was not changed significantly in comparison with the admitted values (
Figure 2).
Mean arterial pressure (MAP) during three days of insulin or metformin treatment. Data were expressed as mean ± SEM
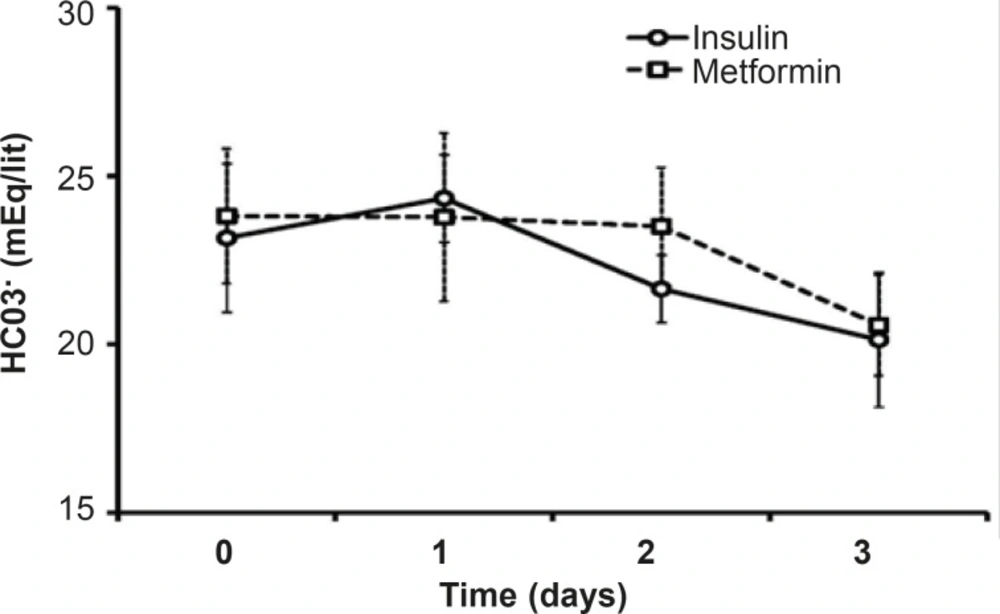
HCO3 and pH
Both pH and HCO
3 did not change statistically during theinsulin or metformin treatment. There is no significant difference between the mean levels of HCO
3in the mentioned groups duringthe treatment days or in each day of treatment (
Figure 3).The mean pH level of metformin treated patients (7.38 ± 0.32) was less than that of insulin group (7.43 ± 0.29), which was not significant.
Changes on HCO3-serum during the treatment with insulin or metformin.Data were expressed as mean ± SEM
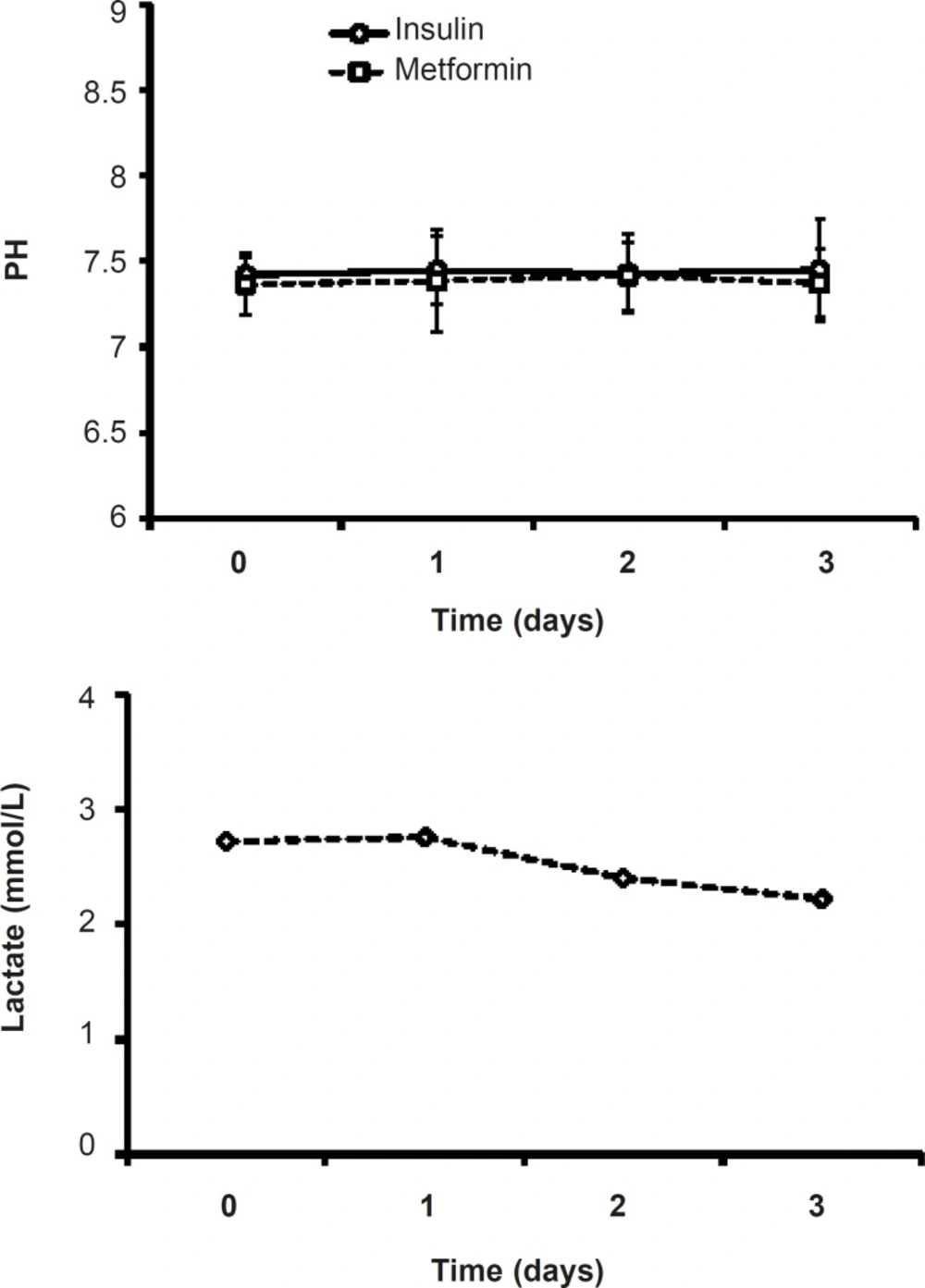
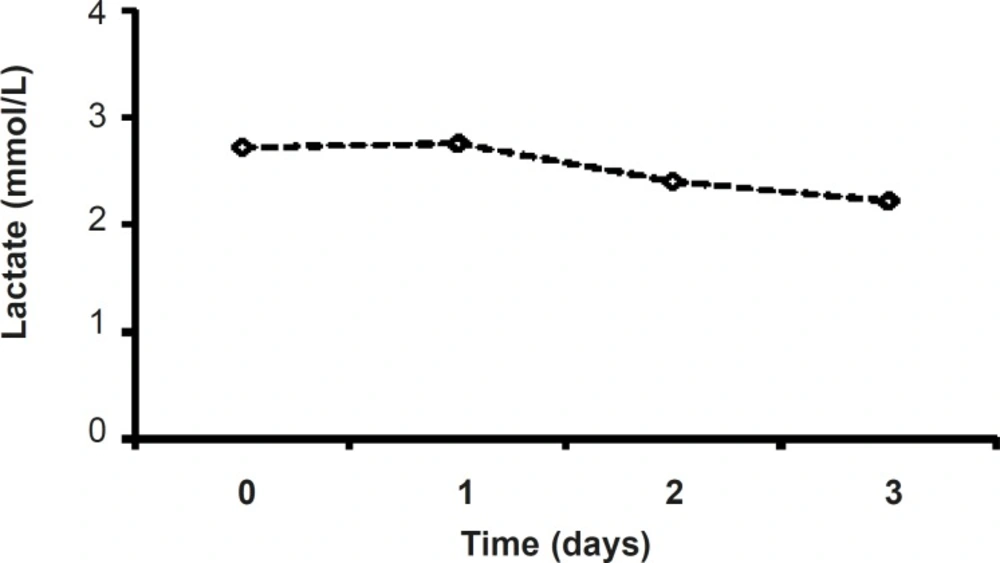
Serum’s lactate in metformin-treated patients
Although in metformin-treated patients, the level of lactate at the end of procedure (2.22 ± 0.31) was less than that of the admitted point lactate value (2.87 ± 0.38), there were no significant changes in lactate values of metformin-related group during the study (
Figure 5). (
Figure 4).
Effects of insulin or metformin treatment on the pH of serum. Data were expressed as mean ± SEM
Serum lactate levels during three days of metformin treatment (1000 mg, twice daily).
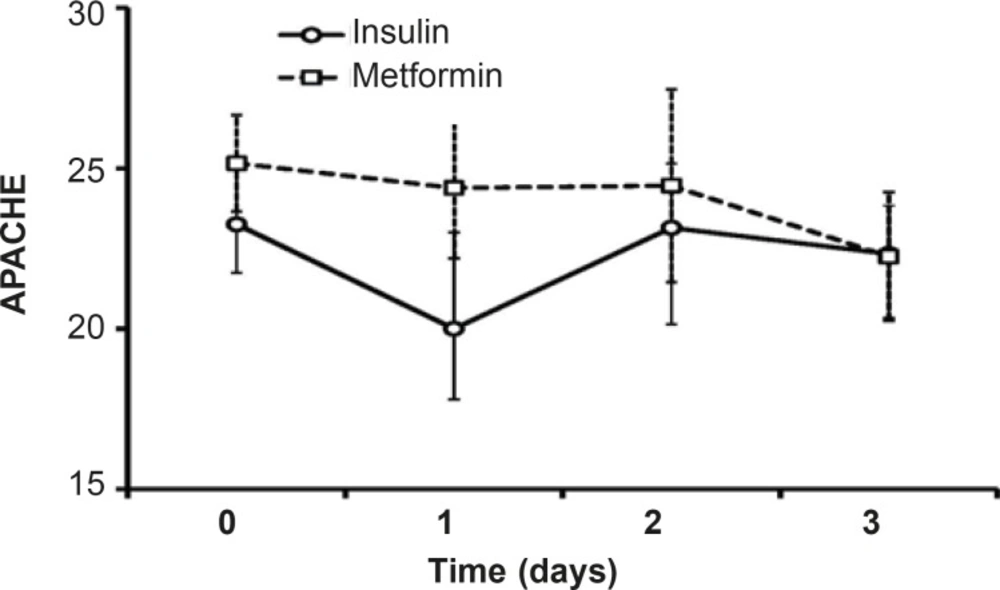
Clinical assessments including APACHE II and G.C.S scale
Along three days of treatment, APACHE II did not change significantly in insulin-treated group or in patients treated with metformin. Although the level of APACHE II in protocol B patients was high than insulin-treated patients, the difference was not significant and afterthree days of treatment, the mean value of APACHE II was the same in both groups (
22.
25,
Figure 6).
Evaluation of APACHE II (acute physiological and chronic health evaluation) as an index of severity of disease in scales between 0 and 71.Data were shown as mean±SEM during three days of insulin or metformin treatment and before the beginning of each treatment (Day 0).
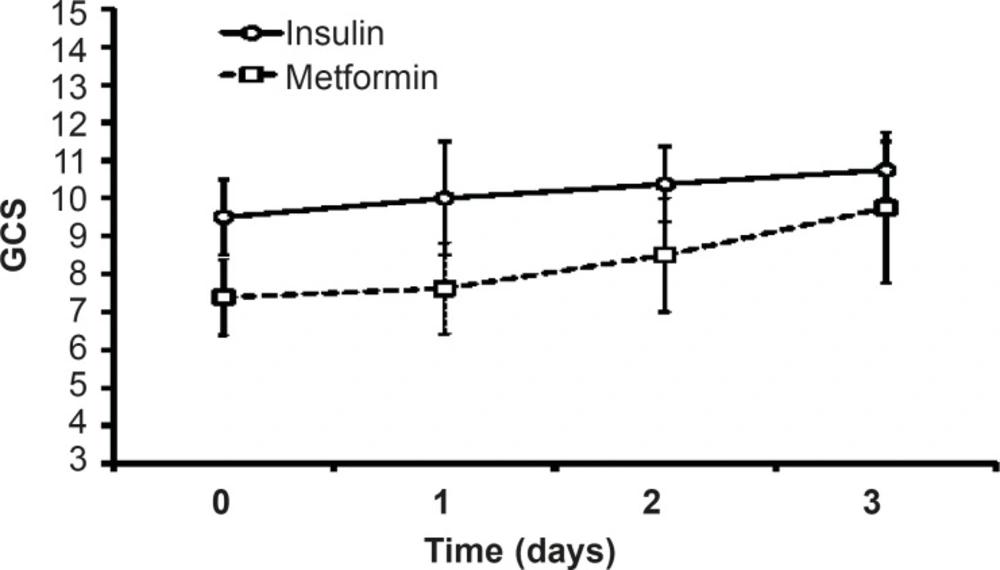
G.C.S value increased after three days of insulin or metformin treatment but there was no significant difference between themin both groups. The value of G.C.S during three days of insulin-treatment was more than the values on metformin-treated patients, but statistical analysis did not showed any significant difference between the groups (
Figure 7).
Glasgow Coma Scale (G.C.S) used for assessing the patients’ consciousness in scales between 3 (deep coma or death) to 15 (complete consciousness). Data were shown as mean±SEM before the beginning of each treatment (Day 0) and during three days of insulin or metformin treatment
Hyperglycemia adversely affects the fluid balance, predisposes patient to infection, and increases the risk of renal failure, polyneuropathy and mortality in ICU (
26). Although it has been reported that low dose metformin therapy improvesthe glycemic control in type 2 diabetic patients (
24,
27),there has been no study so far comparing the effects of metformin therapy with that of insulin on hyperglycemia treatmentin critically ill patients. The currentstudywas aimed tocompare the effects of metformin and intensive insulin administration on the hyperglycemia treatment in critically ill patients for the first time and showed that the metformin treatment reduces BS levels near to normal range. However, there was no difference in MAP, HCO
3 and pH of insulin and metformin-treated patients. Both insulin and metformin treatmentsleaded to non-significant increase in GCS values and decrease in APACHE II.
A recent study on the comparison of metabolic effects of insulin and metformin on patients with severe burn injury greater than 40% of their body surfaceshowed a significant anabolic effect on muscle protein with metformin and a modest response with insulin and suggested that metformin and insulin may work synergistically to further improve on muscle protein kinetics (
28).In present study, metformin therapy reduced the BS levels but could not induce significant change on other evaluated parametersduring the treatment period and results werethe same as insulin.
It has been demonstrated that metformin reduces blood glucose levels predominantly through improving hepatic and peripheral tissue sensitivity to insulin without affecting the secretion of this hormone.It has been shown that metformin does not cause hypoglycemia(
29).Metformin plus insulin appear to lower the incidence of insulin resistance and insulin requirement while maintaining blood glucose level control and consequently lower the incidence of adverse effects related to high-dose insulin therapy, particularly hypoglycemia in patients admitted to ICU(
30,
31). In a study by Ansari G.
et al., patients with systemic inflammatory response syndrome (SIRS) and a blood glucose level of more than 120 mg/dLwere admitted to an ICU received intensive insulin therapy or combination therapy with metformin andthen blood samples were obtained at baseline and at 48 h, 96 h and 7 days after the initiation of study. The results of this study revealed that the addition of metformin to the insulin decreased insulin requirement and concentration of insulin and C-peptide, whereas decreased blood glucose level, therefore lowered the incidence of adverse effects related to the high-dose insulin therapy (
31). A review of study (based on EMBASE and MEDLINE searches from January 1990 to April 2006) done by Staels on two key classes of insulin-sensitizing agents–the biguanides (principally metformin) and thiazolidinediones (pioglitazone and rosiglitazone)–suggested that the thiazolidinediones and metformin, in spite of their distinct mechanisms of action, can provide the clinical opportunity for effective glucose control and metabolic risk reduction (
31).
We did not used combination therapy of insulin and metformin sincethe aim ofpresent study was the comparison of two different treatments separatelyand the resultshowedthat when metformin is used as a single treatment,it canreduce the BS levels. To understand the preciseeffect of single metformin treatment on hyperglycemic patients in ICU, further studies on large ranges of samples and designing advanced protocols is needed.
Lactic acidosis caused by metformin is rare and the risk of this complication may be diminished by the observance of prescribing precautions and contraindications that avoid accumulation of metformin or lactate in the body (
15).Lactateand pH levels did not change significantly during three days of treatment (
Figures 4 and
5) which is a proofthe fact thatmetformin (1000 mg/day)cannot induce lactic acidosis.
In conclusion, compared to the intensive insulin therapy, metformin could not induce a significant change on the experimental parameters or conscious statesof critically ill patients. Although metformin reduced BS levels to desired values along three days of treatment,further studies are neededtoencompass more patients orcombination therapies with insulin or evaluation for a long time todisclose possible clinical insights on reducing the critically ill patients’ mortality.