This is now obvious that cancer progression is related to autophagy, although its exact roles in different steps of cancer progression are not clearly known and it`s also in controversy for some conditions (
13). Regarding the basic difference between tumorigenesis in solid tumors and leukemogenesis in hematopoietic malignancy, the studies deciphering the relation between acute leukemia and autophagy are interestingly growing. Therefore, we aim to find out mentioned relation in acute myelogenous leukemia (AML).
First observation to show a relation between autophagy and cancer was monoallelic deletion of BECN1 gene coding beclin1 in breast, ovary, and prostate cancers. Moreover, another mutations related to autophagy genes in other cancers such as gastric and colorectal were detected (13). Also, LC3 expression in radioresistant breast cancer cells is found intensively different compared to radiosensitive breast cancer cells, and autophagy is considered to be responsible for radioresistant breast cancer cells’ survival (
14). As in a study in 2014, Clioquinol induced mTOR pathway suppression that resulted in autophagy-mediated apoptosis in leukemic and myeloma cells (
15), also it was shown, by Dennis J. Goussetis in 2010, that Arsenic trioxide (A
2O
3) generates anti-leukemic responses in primary progenitors of AML by utilizing autophagy mechanisms
in-vitro (
16).
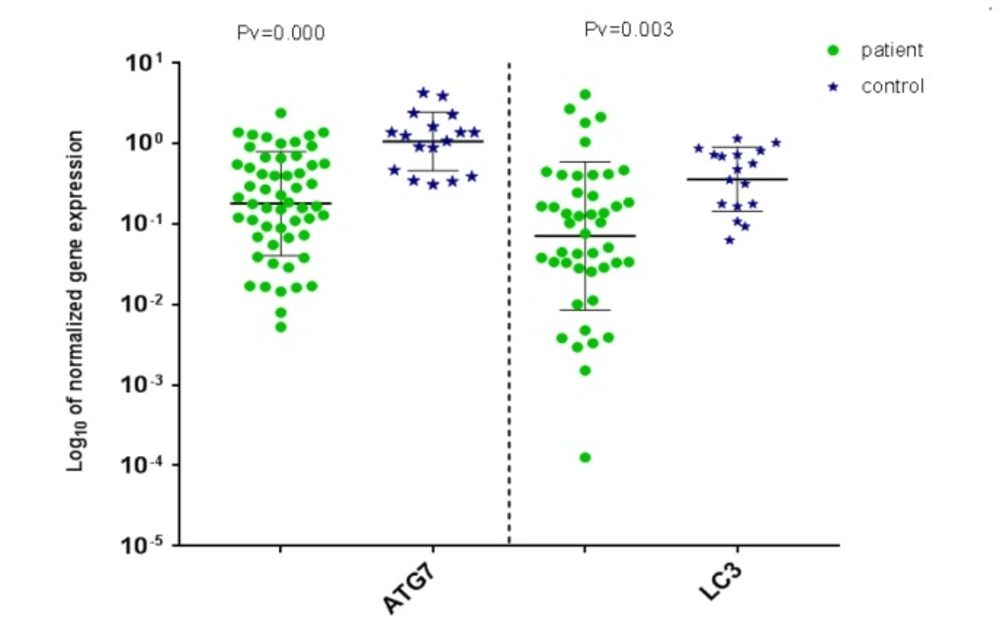
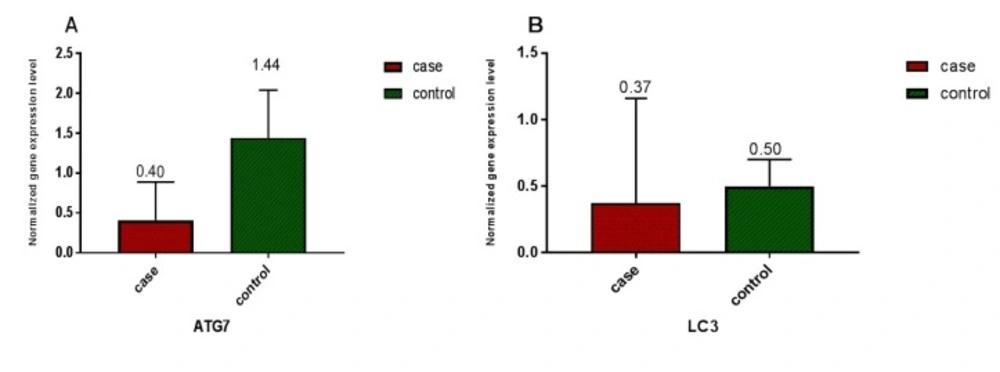
Our results reveal decrease in expression of LC3 and ATG7 genes for majority of de novo AML patients compared to control group, similar as results in study by As Watson in 2015 that showed decreased autophagy gene expression in human AML (MLL-ENL cell line) (
17). So these findings provide possible evidence that the loss of autophagy genes may be generally beneficial for tumor growth, but there are also studies that don’t necessarily support this issue (
18).
Therefore, autophagy expression changes can be valuable in diagnosis, prognosis, treatment targets, and disease monitoring (
19-
21). As we expected, our results mostly show decrease in autophagy gene expression. However, in few patients with gene overexpression and also in some others no significant changes in autophagy genes expression were detected (two parts of the results that in fact led us into new assumption). As we didn′t see similar gene expression levels in all AML patients, this suggests that Leukemogenesis is related to autophagy process in different ways and does not follow a specific pattern.
In many studies autophagy changes were observed in malignancies under chemotherapy and radiotherapy, and they concluded that autophagy genes were overexpressed and resulted in resistance to treatment, so attempted to attenuate autophagy for improvement in treatment outcome (
18,
21,
22). Also, these studies were worked up on refractory patients, in spite of our study on de novo AML patients.
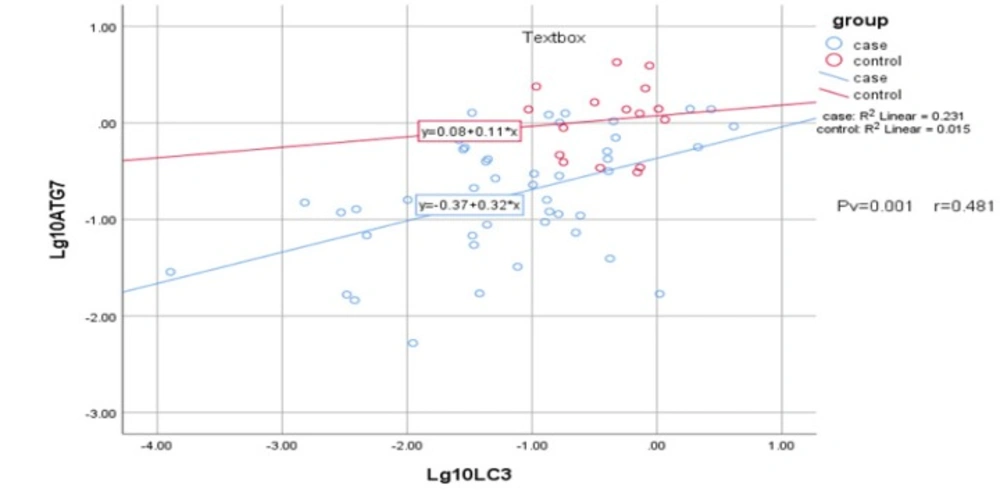
Based on our study, there was no significant correlation between age and these two interested genes expression or between gender and autophagy genes expression. Regarding the decrease in LC3 and ATG7 expression in AML patients compared to control samples and no significant correlation between expression of these genes in AML state as AML-M3 and non-M3 AML, that are naturally different, we suppose that autophagy changes are not directly involved in creating AML by their own, but weakened autophagy mechanisms can be in favor of leukemogenesis.
We conjecture that AML patients who indicated lower expression of autophagy genes during AML onset are as the same patients who are therapy sensitive, owing to their de novo weakened autophagy system; on the other hand those patients who indicated expression of autophagy genes the same as the control sample and also those with overexpressed autophagy genes at the AML onset are the same as the patients who indicate therapy resistance, owing to their intact autophagy system.
Based on our data, in contrast to the current belief that considers autophagy as a double-edged sword and efforts to find answers to the controversial sides of autophagy behaviors, we suppose that in fact fronting with two different faces of autophagy, one as a weakened housekeeping system on the onset of AML and the other face as the origin of resistance to therapeutic procedures, comes from two sides of autophagy in different patients. Actually, we suppose the former ends up with therapy sensitive patients and the latter initiates with the patients of normal or overexpressed autophagy genes.
To prove such a claim another extended study is required to monitor the patients since AML onset till the therapeutic procedure and compare autophagy levels in these two phases of AML together, with the same patients. If such assumption was proved, in future we would be able to characterize our patients into two groups, one as weakened autophagy expression in AML onset accompanied with favor prognosis, and the other as normal or overexpressed autophagy accompanied with poor prognosis. By which we can hope to choose more suitable therapeutic policies in favor of patients.