Herpes simplex keratitis is a relatively common infectious eye disease in the clinic, mainly caused by HSV infection (
13). It ranks first in incidence rate among corneal diseases and may lead to neuropathic pain sequelae, with blindness as a potential end-stage outcome of the disease (
14). Each year, approximately 1.8 million people worldwide contract HSV keratitis, including more than 40,000 new cases that result in severe visual impairment (
15). In addition, it has a high relapse rate after treatment and a long clinical course. For this reason, pragmatic and effective early intervention is of great significance for ensuring the effectiveness of clinical treatment, shortening the clinical course, and reducing the incidence of stromal scarring, astigmatism, neovascularization, ulceration, and perforation (
16).
For patients with an initial outbreak, antiviral treatment is primarily adopted. Ganciclovir, a new type of 2'-deoxyguanine nucleotide drug, is capable of quickly forming triphosphate compounds and specifically binding to giant cells in the body to suppress virus growth (
17). In addition, it can repress the replication of viral DNA by competitively inhibiting herpes-zoster virus DNA polymerase and reducing the binding of herpes-zoster virus DNA to nerve cells (
18,
19). Ganciclovir has certain value for treating new cases, but ganciclovir treatment alone is associated with frequent recurrence after treatment and even post-stage neuropathic pain complications (
20).
A study (
21) found that C5, an inflammation-related factor, has immune regulatory functions, with an overtly raised expression in many immune diseases, including the HSV immune response. C5 is a chemokine for various inflammatory cells and can effectively promote the fusion of lysosomes and cell membranes, playing an important role in the body's immune response. Moreover, it can also induce the production of various inflammatory cytokines, including TNF-α and interleukin-1, activate the NF-κB signaling pathway, and enhance the aseptic inflammatory response, thereby aggravating damage to tissues and cells (
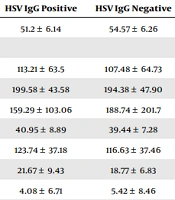
22). In this study, ganciclovir gel was adopted in the control group, while PSDS combined with ganciclovir gel was used in the ganciclovir + PSDS group to treat HSK. Serum C5 concentration in the ganciclovir + PSDS group was markedly lower than that in the control group at 3, 7, and 10 days after treatment, suggesting that PSDS combined with ganciclovir is able to effectively decrease serum C5 concentration in HSK.
In addition, the concentrations of hs-CRP, TNF-α, MDA, and SOD in both serum and tear fluid were lower in the ganciclovir + PSDS group compared to the control group after treatment, implying that PSDS combined with ganciclovir can effectively reduce both inflammatory responses and oxidative stress in HSK patients. Furthermore, the change in C5 concentration had a positive correlation with the change in hs-CRP concentration and a negative association with the change in SOD concentration in the serum and tears, indicating that changes in C5 concentration are robustly associated with changes in the inflammatory and oxidative stress markers. Furthermore, the time to clinical symptom improvement was compared between the two groups, and it was found that the time to improvement of eye dryness and pain, corneal wound healing, and lacrimation in the ganciclovir + PSDS group was considerably shorter than that in the control group. This suggests that PSDS combined with ganciclovir is capable of effectively mitigating the clinical symptoms of patients.
Subsequently, in comparison with the control group, the ganciclovir + PSDS group displayed a longer tear film BUT, a higher corneal fluorescence staining score, a larger volume of tears secreted, and a higher TMH, implying that PSDS combined with ganciclovir in the treatment of HSK can effectively improve tear properties. Lastly, the clinical efficacy was found to be superior in the ganciclovir + PSDS group. The remission rate was higher in the ganciclovir + PSDS group than in the control group, and the ineffectiveness rate was lower in the ganciclovir + PSDS group than in the control group. These findings further indicate that, for HSK, PSDS combined with ganciclovir may provide considerable improvements in clinical efficacy.
Ganciclovir alone, applied for the treatment of HSK in this study, is capable of effectively suppressing viral infection, with high safety and fast onset. However, it had no obvious effects on improving inflammation or oxidative stress or in reducing relapse. As an extract of potassium sodium salt from andrographolide succinic acid, PSDS, used in the ganciclovir + PSDS group, can effectively enhance the resistance and immunity of the body (
23). Additionally, it can lower capillary permeability, inhibit inflammatory responses, reduce tissue edema, and improve the activity of peripheral neutrophils and macrophages to some extent (
24).
In vitro tests (
25) have shown that PSDS can effectively kill multiple viruses, such as adenovirus, HSV, respiratory syncytial virus, and rhinovirus, and also has a certain inhibitory effect on various pathogenic bacteria (
26). Potassium sodium dehydroandroandrographolide succinate combined with ganciclovir gel in treating HSK significantly cleared the virus and reduced inflammation and oxidative stress (
27). The strengths of our study are the detailed assessment of clinical outcomes and the mechanistic evaluation of inflammatory and oxidative stressors, including the novel finding of C5 as a marker of the HSK course. This is the first study to report the potential efficacy of ganciclovir in combination with PSDS for the treatment of HSK.
However, this was a preliminary clinical study, which entails several limitations. First, the doses of ganciclovir gel were mismatched between the groups, with the ganciclovir + PSDS group receiving a lower dose during the 10-day treatment period. Second, the results of the study were limited to a 10-day treatment period, and certain clinical outcomes were subjective and variable, potentially affecting the assessment of efficacy. Future studies need to use standardized and objective measures to assess efficacy over longer follow-up periods and account for potential long-term side effects. Third, an initial sample size calculation was not performed. However, post hoc power analyses indicated that in independent samples t-tests and χ² analyses with 40 individuals per group, we had 80% power to detect a moderate effect size of 0.6 (Cohen’s d).
Fourth, because the study focused on potential anti-inflammatory mechanisms of action, viral load was not tested, and the impact of treatment on antivirals could not be assessed. We hope that the current preliminary results will stimulate interest in initiating and designing larger clinical trials to determine the efficacy of PSDS for HSK treatment. In addition, although biochemical indices in serum and tears provide new insights into assessing the clinical efficacy of PSDS in HSK, they still need to be supported by a large number of high-quality clinical and laboratory studies to confirm their validity and utility as surrogate endpoints. Future studies should aim to establish a strong link between these indices and clinical outcomes of PSDS for HSK.
5.1. Conclusions
In conclusion, the serum C5 concentration of HSK patients was significantly elevated and was closely related to inflammation and oxidative stress factors. The application of PSDS combined with ganciclovir effectively reduced the concentration of C5, inhibited the inflammatory response, enhanced the body’s antioxidant capacity, and significantly improved the clinical symptoms of the patients, with better efficacy than ganciclovir alone.



 concentration")
 concentration")
 concentration in tear fluid")
 concentration in tear fluid")