Trunk muscles’ size and function have received much attention in the literature considering their role as a risk factor for LBP in the general population and also in athletes (
6-
8,
24). Whether truck muscles’ size could be a cause for LBP in athletes, such as soccer players, was our question and led us to design the present study. This study’s findings revealed that LBP incidence (18.91%) in elite male soccer players was not directly associated with lateral abdominal muscles’ thickness, CSA of LM, hamstring flexibility, isometric endurance of trunk extensor, back muscles’ flexibility, and leg length discrepancy during the one season follow-up period. Alteration in these factors may be responsible for LBP recurrence, and its investigation is suggested for future studies.
The incidence of LBP in elite soccer players was estimated to be near 19 percent (7 out of 37), or 1.13 non-traumatic injuries per 1000 training hours, in this 6-month cohort study. In the literature, few studies have evaluated the incidence of LBP injuries in athletes. In the study of Haydt et al. (
25), the incidence of LBP was reported at about 56% (50/90) in 90 female field hockey players between 18 and 24 years old. On the other hand, Newlands et al. (
26) revealed the LBP’s incidence near 1.78 injuries per 1000 training hours in elite rowers. Also, Walden et al. (
27) illustrated that the incidence of LBP in northern and southern groups of professional European football clubs was about 0.20 and 0.10 injuries per 1000 exposure hours, respectively, during the nine-season prospective cohort study. Besides, Mueller et al. (
28) mentioned that the incidence of LBP is about 15% in adolescent soccer players. Moreover, Hangai et al. (
29) reported that in soccer players, the LBP odds ratio is approximately 1.6 (CI: 1.3 - 2.2). Some of these studies have reported traumatic and non-traumatic injuries separately; others have not differentiated the injuries. Therefore, the inconsistency between the incidence rates of LBP could be due to different studies’ participants, injury definitions, and follow-up periods.
Overweightness and obesity have been suggested as risk factors for LBP in athletes (
4). Similarly, the mean BMI and height of the participants, who experienced LBP in our study, were higher compared to the asymptomatic players (BMI = 22.03 ± 1.21 vs. 21.6 ± 1.15), (height = 179.07 ± 3.72 vs. 175.96 ± 8.30). However, the statistical relation between LBP and BMI was not statistically significant. In contrast, the case-control study by Grosdent et al. (
30) illustrated a significant relationship between LBP and BMI among soccer players with and without LBP (BMI = 22.6 ± 1.6 vs. 21.2 ± 1.3), (height = 182.2 ± 7.3 vs. 177.3 ± 5.3). Even though the BMI and height differences between the mentioned studies were similar, the number of participants was balanced between the two groups (with LBP and without LBP) in the latter study, and it could be the reason for the significance of the results.
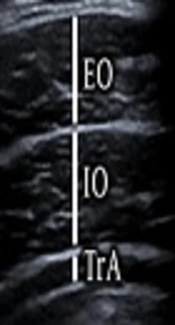
The thickness of trunk muscles (TrA, IO, EO, and LM), which have been measured by the ultrasonography method in both resting and contraction positions did not show a statistically significant difference between players with or without LBP at the baseline of this cohort study. Previous studies have shown that there is a relationship between LBP and trunk muscles’ size and contraction ability in different athletes (
6,
31). In the study of Hides et al. (
6), the CSA of the trunk at the L3-4 disc level was measured by using magnetic resonance imaging (MRI), at the beginning and end of the drawing-in maneuver in Australian footballers with LBP. Their results illustrated that there was a significant decrease in the CSA of the trunk in athletes with LBP (
6). Also, Hides et al. (
6) revealed that in elite soccer players with LBP at the start of the preseason, CSA of LM at L4-L5 level was lower in comparison with players without LBP, and with decreasing the LBP, the CSA of LM was improved (
31). The thickness of IO and TrA muscles in contraction were improved significantly in elite cricket players, with and without LBP, who participated in a staged core stabilization training program (
32). This cohort study was conducted for assessing the role of trunk muscles’ thickness in the incidence of LBP, and its findings could not confirm the role of these muscles’ thickness as a risk factor for the development of LBP in elite soccer players. It could be hypothesized that after experiencing an episode of LBP, possibly due to disuse or changes in trunk neuromuscular control, the thickness of these muscles decreased, which led to the recurrence of LBP later. Considering the fact that cross-sectional studies cannot investigate the cause and effect relationship between several variables; the contradiction between our study and previous studies could be due to the different designs of these studies.
Furthermore, hamstring flexibility, back flexibility, and back muscles’ endurance (Sorensen test) did not differ between the two groups in this study. In the study of Rostami et al. (
7), the lower thickness of TrA and CSA of LM was observed in cyclists with LBP compared to cyclists without LBP. In the same study, no relation was detected in the isometric back strength of the athletes with LBP compared to the ones without LBP. In accordance with our study, Moradi et al. (
4), in a systematic review, found insufficient evidence for a possible relation between the forward bending (which consists of both hamstrings) and back flexibility.
Considering the findings of the studies accomplished so far, there are many gaps in discovering the etiology of LBP in soccer players. To the best of our knowledge, this study is the first cohort study designed to discover the effect of lateral abdominal muscles’ size and CSA of LM as risk factors of the incidence of LBP in adult soccer players. As mentioned previously, most of the previous studies on athletes’ LBP are based on a cross-sectional design that has several limitations, such as not specifying causal relations, or in other words, an unclear direction from risk factors to outcome. These studies mainly show an association with no specific cause and effect relation. Furthermore, in such studies, the process leading to a disease/disability or the causal factors mentioned as risk factors rest in the past. Together, the aforementioned limitations increase the value of the present study because cohort studies are designed to discover causal links between possible risk factors and outcomes (cause and effect relationships). It is possible that a cohort study can reject the findings obtained by cross-sectional studies. As results in the present study show, there may be an opposite direction between the relation of LBP and trunk muscles’ thickness. It seems that while some studies consider the effectiveness of various movements in the activation of trunk muscles and prevention of low back pain (
33,
34), this study could not support the role of these muscles in the incidence of low back pain in male soccer players. Maybe other factors such as overtraining and psychological factors should also be investigated in parallel (
35).
As the present study is aimed to explore the etiology of LBP in soccer players, it can be considered as a base for further longitudinal studies. Indeed, we need to establish a standard protocol (valid and reliable) for future cohort studies. Based on the findings from our literature review and also observations, we summarized some recommendations to improve the quality of future studies examining the incidence and probable risk factors of LBP in athletes:
The definition of LBP should be clear and exact, and the same definition should be used in all related studies. A standard definition could be “low back pain is pain between the last rib and lower gluteal fold, which is bad enough to limit or change athletes’ daily routine or sports activities for more than one day” (
2).
For more generalizability in cohort studies, following a large sample size considering both genders could be more effective regarding loss to follow-up ratios.
Long term follow-up (at least one year), which covers pre-season, in-season and off-season periods can be more reliable for discovering risk factors in different spans of athletes’ sports history. According to the previous studies, overuse and traumatic injury during a season (
31) and in off-season periods, different lifestyles, and training can affect the incidence rate of LBP in athletes.
Investigation of other outcomes beyond LBP incidence, such as neuromuscular injuries and performance could be beneficial.
Evaluation of possible markers involved in LBP could be useful during cohort studies to detect possible mechanisms of LBP.
Measurements such as ultrasonography method and further functional assessments should be done under standardized protocols (see previous references in method) to minimize errors.
It would be better if measurements are performed consecutively (e.g., every week or month) during follow up periods in case of detecting any LBP incidence and related changes in muscles’ size or physical function.
Detection of intrinsic risk factors of LBP (including weight, BMI, change in lumbar range of motion, hip flexor tightness, previous history of LBP and participation in more than one type of sports) and other probable extrinsic risk factors (such as duration of participation in competitive sport, training hours per week and playing position and the type of field, e.g. natural vs. artificial grass) should be evaluated before and during the study (
4).
The recurrence rates of LBP during the follow-up period should be evaluated with possible causes.
The effect of different sport-specific movements such as dribbling, jumping, heading during soccer could be considered as risk factors for LBP, and their evaluation could be helpful.
Qualitative studies based on individual interviews with the athletes could further help in discovering the possible mechanisms of LBP in soccer players.
This study aims to cover these considerations as much as possible; however, it has several limitations including studying male players which could affect the generalizability of results, and short follow-up period (only a one-season period), which may have affected the results. Besides, we did not evaluate the type of playing field and participation in other sports. To minimize loss to follow-up of participants, free of charge therapeutic services were offered to players during the follow-up period. Furthermore, the participants were assured that the study’s data would be confidential and only the examiners had access to it.
5.1. Conclusions
While seven participants (18.91%) experienced LBP during the follow-up period, this study showed that soccer players who experienced LBP during the study had no statistically significant differences in their baseline characteristics including abdominal muscles’ thickness, CSA of the LM, hamstring flexibility, back flexibility, muscle endurance, and leg length.