1. Background
Jump landing is a complex but common movement in sport activities. Volleyball and basketball games require jumping and landing tasks. While competing and practicing, athletes frequently perform multi-planar jump landing. Lower extremity biomechanics have exhibited significant differences among various directions of jump landing (1-3). Sinsurin K et al. (2, 3) found that single-leg landing in diagonal and lateral directions showed higher peak knee valgus and less knee flexion angle at initial contact than the forward direction. They suggested that lateral and diagonal jump landing could lead to risk of knee injury.
Anticipatory muscle activity could influence the amount of knee flexion and prepare the knee for dynamic weight bearing such as landing tasks. This muscle activity represents pre-programmed muscle control to dampen the impact forces (4). Impact forces have been shown to be absorbed by the muscles rather than non-contractile joint and ligamentous structures (5). High preparatory muscle activity helps reduce the time needed to develop muscle tension when the landing occurs. The linear proportion of the active muscle tension and the tensile stiffness was observed (6). By increasing sensitivity of muscle spindle, an enhancing alpha-gamma co-activation was noted to increase the joint awareness, to increase muscle stiffness, and to prevent joint injury during decelerated movements (4, 7, 8). Less unexpected knee movements during landing should result with high preparatory muscle activity (8, 9). Therefore, greater control of landing may reduce the risk of ligamentous injury. Muscles around knee joint play a major role in controlling the knee displacement during movements. Then, we were interested in knee muscle functions and would like to know that how an athlete familiar with jumping naturally responds during multi-direction jump landing.
Landing with less knee flexion angle might increase the risk of ACL injury because of the greater knee extensor load (10, 11). Some studies reported an increase of knee flexion excursion during landing as a strategy to reduce the risk of knee injury (12, 13). Increasing knee flexion excursion during landing decreased forces and movements at the knee joint resulting an increase in time from initial contact to peak knee flexion (14). Knee flexion displacement or excursion was the second outcome, in which we were interested to observe how an athlete responds during multi-direction jump landing.
2. Objectives
The purpose of the present study was to examine the knee muscle function and flexion excursion during landing in various directions. It was hypothesized that athletes might prefer the strategy of increased knee muscle activity and knee flexion excursion to prevent knee injury during diagonal and lateral landing. This study would provide information of knee biomechanics during jump landing in various directions. Findings could be linked to how to land with appropriate movement.
3. Materials and Methods
Eighteen male athletes participating in the basketball and volleyball teams in the organized university level were recruited (mean age 20.2 years, range 19 - 24 years, mean body mass index 22.31 kg/m2, range 20.34 - 24.91 kg/m2). Inclusion criterion was participating at least 3 times per week for at least 3 months in the game or practice prior to testing. No participant had musculoskeletal disorders within 3 months prior to data collection. The exclusion criterion was a history of serious injury or operation of lower extremities (e.g., ACL injury, fracture, patellar dislocation). All participants provided written informed consent before the experiment. The committee on human rights related to human experimentation of Mahidol University approved this study.
This study was conducted at the human performance laboratory at the Faculty of Physical Therapy, Mahidol University. A ViconTM 612 workstation (Oxford Metrics, Oxford, UK) comprising infrared cameras was used to collect the kinematic data at sampling frequency of 200 Hz. The sixteen reflective markers based on lower body model of Plug in Gait were placed bilaterally on the subject’s bony prominences at the anterior superior iliac spine (ASIS), posterior superior iliac spine (PSIS), thigh, lateral condyles of femur, shank, lateral malleolus, heel, and 2nd metatarsals. AMTI forceplate was synchronized with the ViconTM Motion system in order to determine the initial contact of landing phase.
Muscle activity was recorded by an electromyography (Noraxon Myosystem) at a frequency of 1000 Hz, which was synchronized with the ViconTM Motion system in order to quantify dynamic muscle function of vastus medialis (VM), vastus lateralis (VL), rectus femoris (RF), semitendinosus (ST), and biceps femoris (BF). The skin preparation over the bellies of muscle included shaving, abrading, and cleaning the skin with alcohol prior to electrode application. Inter-electrode impedance was less than 10 kiloohm. Cable sway was minimized by the use of adhesive tape. Surface electrodes were placed in pairs over the VM, VL, RF, ST, and BF muscles in dominant leg with an interelectrode spacing of 2 cm center to center according to recommendations of the European Recommendations for Surface Electromyography (www.seniam.org). The dominant leg was identified based on the preferred leg when performing a single- leg hop for a distance (15).
Multi-direction jump-landing tests composed of four directions including forward (0°), 30° diagonal, 60° diagonal, and lateral (90°) directions. Participants were asked to jump from a 30 cm height wooden platform and land on the center of AMTI forceplate without falling. Three successful trials of jump landing in each direction were recorded. The research setting and complete details of the jump-landing protocol has been reported elsewhere (3).
Second order recursive Butterworth filter was used for filtering the EMG data. EMG data from each muscle was filtered at low pass frequency 350 Hz and high pass frequency 30 Hz, respectively, and then, full-wave rectified. The high-pass corner frequency was determined from De Luca. In vigorous and spastic muscle activity, the corner frequency should be increased above 20 Hz (16). The averaged EMG data was the primary outcome, which represents the muscle function to control tibial segment on femural segment. It was collected between 100 ms prior to foot contact and 300 ms after foot contact and normalized to percentage of maximum EMG amplitude during forward jump landing. Maximum EMG was calculated from the highest 20 ms muscle activity in the forward jump-landing trial. The purpose of maximum EMG was to normalize between jump-landing directions.
Sixteen marker coordinates were filtered by a fourth-order zero-lag Butterworth digital filter at cut-off frequency of 8 Hz. The cut-off frequencies were determined using the residual analysis technique (17). Knee flexion angles during jump landing were obtained after the lower extremity model was constructed by the Plug-In Gait software. Knee flexion excursion was the secondary outcome, which represents the knee joint displacement responding to the external impact forces. Increasing knee flexion excursion during landing decreased forces and movements at the knee joint resulting less risk of knee injury. It was calculated as the difference between the knee flexion angle at foot contact and the peak angle of knee flexion during landing (18).
Data tested by Kolmogorove-Smirnov Goodness of Fit Test was normally distributed. The statistical comparisons were performed with SPSS statistics 17. One-way repeated measures ANOVA was used to compare the main effect of direction. Pairwise comparisons were performed with Bonferroni correction. The level of statistical significance was set as a p-value less than 0.05.
4. Results
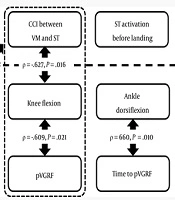
RF and ST muscle activities showed significant differences (P < 0.05) in 100 ms before foot contact (Table 1). From forward to lateral directions, RF and ST exhibited a trending increase and decrease of muscle activity, respectively. After foot contact, VL and RF muscle activities showed significant differences (P < 0.05) (Table 2). Jump-landing direction significantly influenced (P < 0.001) knee flexion excursion (Figure 1). Less knee flexion excursion was observed in lateral landing compared to diagonal and forward jump landing.
Comparison of average knee flexion excursion during landing among four directions of jump landing. Asterisk indicates statistical significance between jump-landing directions (P < 0.05).
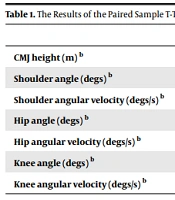
Table 1. Comparison of EMG 100 ms Before Foot Contact Among Various Directionsa
aValues are expressed as mean (SD).
bStatistically significant difference compared with lateral direction (P < 0.05).
Table 2. Comparison of EMG 300 ms After Foot Contact Among Various Directionsa
aValues are expressed as mean (SD).
bStatistically significant difference compared with lateral direction (P < 0.05).

Figure 1.
Knee Flexion Excursion During Landing
5. Discussion
The present study investigated the knee biomechanics including the knee muscle activity and knee flexion excursion in order to observe how an athlete familiar with jumping naturally responds during multi-direction jump landing. Our findings show that (a) muscle activity was significantly different in the different jump-landing directions, specifically the RF and ST muscle activities before foot contact and VL and RF muscle activities after foot contact, and (b) knee flexion excursion during landing indicate a decreasing trend from forward to lateral jump landing.
5.1. EMG 100 ms Before Foot Contact Among Various Directions
Preparatory muscle activity is controlled by the central nervous system through feed-forward and internal feedback (proprioception) mechanisms (19). Previous studies suggested that preparatory muscle activity was more important to prevent excessive knee valgus motion than reactive muscle activity after foot contact (4, 20). This study showed a significant direction effect of EMG of ST muscle in 100 ms before foot contact. This might be a pre-programed motor command that responds differently to different directions of the jump. Palmieri-Smith RM et al. (4) reported that peak knee valgus angle (PKVA) during landing was positively associated with the EMG activities of VL and lateral hamstring muscles. But found that high preparatory muscle activity of VM was negatively associated to PKVA. It could be that the lateral knee musculature would create the knee valgus that should be counteracted by the medial knee musculature such as vastus medialis and medial hamstring muscles. High activation of the lateral thigh muscles would associate with the risk of ACL injury. This pattern of activation was found in female athletes that were different from male athletes (21, 22).
Less activation of knee flexor muscles before landing might increase the risk of ACL injury. Chappell et al. (23) reported an increased activity of knee flexor muscles before an unexpected landing. This is a pre-programed motor command in the knee flexor muscle group acting as a preparatory mechanism for immediately responding to loading at impact. It might indicate that lateral jump landing with less ST muscle activity has higher risk of knee injury than other directions in this study.
Aggressive forces of quadriceps muscle could induce excessive ACL tension during slightly knee flexion (24, 25). RF preparatory muscle activity showed an increasing trend from forward to lateral direction in this study. Force from RF muscle directly pulls the tibia and induces anterior tibial translation. There was an opportunity of greater anterior tibial translation in lateral jump landing. This study indicated that RF muscle was increasingly activated in diagonal and lateral directions of one-leg jump landing which might be an unfamiliar direction of jump landing.
Therefore, neuromuscular training for muscles around knee joint should be focused on for responding in multi-direction jump landing, especially enhancing VM and ST muscles. The appropriated preparatory muscle function could prevent the awkward lower extremity posture at foot contact, which could lead to injuries (23).
5.2. EMG 300 ms After Foot Contact Among Various Directions
From forward to lateral direction, this study showed a non-significant trend of increasing activity of ST and BF muscles 300 ms after foot contact. In 2008, Wikstrom et al. investigated EMG activity of VM and SM (semi-membranosus) muscles during multiple jump-landing directions (26). They reported no significant differences in mean EMG activity before and after foot contact between sagittal, diagonal, and lateral jump-landings. They suggested that jump landing in multiple directions did not induce a pre-programed motor command differently. However, the present study included more muscles and found a significant difference of some muscles in both preparatory and landing phases (Tables 1 and 2). Our findings also showed no significant difference of ST and BF muscle activities. A needed ST and BF muscle activity was observed in lateral direction of jump landing. This might be the strategy of knee flexor muscles during landing in various directions.
Lower extremity flexion during landing can help to prevent ACL injuries because impact loading is distributed by the contractile structure. The force from hamstring muscle contraction is efficient in more knee flexion due to an association between a greater perpendicular tendon and tibial shaft angle (27, 28). In addition, the hamstring muscles play a role in controlling tibia rotation. Medial hamstring and BF can prevent excessive external and internal rotation of tibia bone, respectively (29). Sinsurin K et al. (3) found that single-leg landing in lateral direction showed higher PKVA than diagonal and forward directions. Neuromuscular response is an important factor in increasing joint dynamic stability and preventing injuries (30). The contraction of muscle around knee joint can reduce knee valgus motion (31, 32). Higher muscle activity in BF and ST muscles during lateral landing was found in this study. This might be the cause of increasing muscle activity in BF and ST in order to reduce knee valgus loading.
5.3. Knee Flexion Excursion During Landing
An increase of knee flexion excursion during landing could be a strategy to reduce vertical ground reaction forces during landing. A trend of decreasing knee flexion excursion was observed in the forward, 30° diagonal, 60° diagonal, and lateral landing, respectively. In contrast with a previous report, a significant increase of knee flexion angle at initial contact was noted from forward, 30° diagonal, 60° diagonal, and lateral jump landing (2). It is possible that the jumpers preferred strategy with higher knee flexion angle at initial contact and less knee flexion excursion during landing in diagonal and lateral jump landing. However, this strategy might result in an increased risk of ligamentous injury. Onate et al. (12) found that a decrease of peak ground reaction force was shown after the jumper received instruction on proper landing technique. Jumpers landed with greater knee flexion angle and increasing knee flexion angular displacement. These findings suggest that the landing movement can be altered with training a particularly important consideration during landing in more lateral directions to reduce the risk of knee injuries.
The present study exhibited that multidirectional jump landing affects the knee muscles activity and knee flexion excursion. The current study examined and reported muscle activities of the knee in healthy athlete groups. So, the data might be representing the natural patterns of the knee muscles in various jump-landing directions. However, jump-landing tests in the present study were performed in the laboratory. Application of the finding to the real situation should be interpreted carefully. For further study, it is interesting to study more in more muscles and participants with knee problem.
5.4. Practical Applications
A higher risk of knee injury might occur during lateral jump landing than forward and diagonal directions. Athletes should have more practice in jump landing in lateral direction to avoid injury. Landing technique with high knee flexion in multi-directions should be taught to jumpers for knee injury prevention.