Pulmonary cystic lesions are defined as gas-containing translucent areas with a wall thickness of ≤ 4 mm. On the other hand, a cavitary lung lesion is defined as a gas-containing translucent area with a thicker wall than cystic lung lesions (> 4 mm) (
8,
9). Although cavities are commonly seen in lung cancer patients, accounting for 22% of all primary lung carcinomas (
9), thin-walled cystic lung cancer has been rarely reported in the literature. Cavitary lung cancer is common in patients with squamous cell carcinoma (SCC) and is often seen in adenocarcinomas (
10). Occasionally, it can be found in bronchioloalveolar carcinoma (BAC), while small-cell lung cancer has not been associated with cavitary lesions (
10).
Today, formation of gas-bearing lacunae is believed to occur through several mechanisms: (1) tumor tissue invasion of the original lung cyst or bullae; (2) ischemic necrosis of tumor tissue and excretion of the liquefied part through the bronchus to form a cystic translucent area; and (3) one-way valve formation. According to the characteristics of patients in the present study, as well as previous publications, one-way valve formation is believed to be the main mechanism of cystic lung cancer development with peripheral GGO.
The evolution of GGO lesions from atypical adenomatous hyperplasia (AAH) to adenocarcinoma in situ (AIS) and to minimally invasive adenocarcinoma (MIA) is an evolving and progressive process. As it further infiltrates the lung tissue, tumor invades the alveolar wall, bronchiolar wall, and interstitial lung, forming a one-way valve that continuously accumulates gas in the alveolar space. Multiple alveolar spaces then burst and fuse into a cystic cavity; over time, pressure inside the cyst increases, and its volume expands.
The epidermal growth factor (EGFR) is believed to be involved in multiple processes, such as tumor infiltration, angiogenesis, and cell proliferation (
11). A previous study reported that 81% of all thin-walled cystic lung cancers are associated with EGFR overexpression (
12). In the present study, 18 (75.0%) tumors were reported in the upper lobe of the lungs, as the preferred site for emphysema. Although tumor tissue invasion into the existing pulmonary cysts or large bulla structures has been proposed in the literature, this theory cannot be widely accepted, since lesions have not been found in the common sites of bullae, and this type of balloon-containing lumen has not been previously observed (
13).
Some researchers believe that the soft and fragile nature of tumor tissue leads to the elastic retraction of the peripheral lung tissue and aggravates the valve mechanism (
14,
15). Microscopic analyses have indicated tumor infiltration along the walls of the bronchioles and cyst, but not the liquefied necrotic tissue. This observation better supports the mechanism of one-way valve formation in thin-walled cystic lung cancer, which is completely different from the mechanism of cavity formation in necrotic tumors, such as SCC.
In the present study, 14 out of 24 patients (58.3%) showed fine partitions or small blood vessel shadows in the cavity, suggesting cavity formation as an expansion-like change, as cavitary lung cancer does not show partition opacity due to complete liquefied necrosis. Since GGO lesions have the characteristics of malignancy, such as lobulation, vascular convergence, pleural depression, and burr signs, thin-layer CT scan and MPR can reflect these imaging features completely to indicate the exact location of the lesion, the size of the cavity, and the relationship of these lesions with peripheral tissues. Therefore, CT imaging is the preferred method for examining thin-walled cystic lung cancer with GGO.
Since it is difficult to distinguish between benign and malignant parenchymal lesions, fiberoptic bronchoscopy and percutaneous lung biopsy are suggested for pathological diagnosis. Considering the characteristics of thin-walled cystic lung cancer, its pathology may be challenging because of thin walls. Also, as inaccurate puncture can easily lead to pneumothorax. Some scholars have proposed the application of CT-guided percutaneous needle aspiration biopsy to avoid this complication (
16).
Cavitary lung lesions may be associated with some diseases. They are commonly seen in SCC patients. The pathological mechanism of this type of cavitation involves the formation of liquefied tumor necrosis that creates a hollow area through bronchial discharge, forming a thick-walled cavity with an irregular internal surface. Wall nodules without internal partitions or vascular structures and lobulation signs may be also present. Besides, pleural depression, burr sings, and other malignant signs may be observed.
Moreover, pulmonary cysts or bullae are identified as thin-walled lung cysts. Internal partitions, lobulation signs, wall nodules, and other signs are absent in these cysts. During alveolar expansion, cystic cavity develops through rupture and fusion of the alveolar wall, usually caused by obstruction of a small bronchial valve. Besides, tuberculosis cavities mainly present as fibrous thick-walled cavities with extensive cord-like fibrotic changes around the lesions, scattered new and old lesions, calcification, pleural thickening, and other symptoms. Once Mycobacterium tuberculosis is found in clinical sputum samples, identifying the disease is not difficult.
In this study, we reviewed the clinical and radiographic features of 24 patients with thin-walled peripheral GGO. The findings showed that most cases of lung cancer were adenocarcinomas. In terms of imaging features, 50% of the lesions showed pure GGO, while 50% showed mixed GGO. Most of the lesions were associated with at least one sign of lobulation, burr sign, vascular convergence, or pleural depression. With a pathological understanding of the MSCT features of thin-walled cystic lung cancer with GGO, benign and malignant cases can be distinguished when encountering similar images (
3).
Considering the prognosis of thin-walled cystic lung cancer, studies in the literature have reported small sample sizes with limited survival data. In our dataset until June 2020, 16 patients expired, while eight patients remained alive during the follow-up (39 - 69 months), with a three-year survival rate of 33.3%. However, the survival rate was reported in a small sample size (n = 24), and further validation in a larger sample size is needed for survival studies. Therefore, similar cases should be examined, and prognosis needs to be further evaluated.
In conclusion, thin-walled cystic lung cancer with GGO is a rare clinical phenomenon. Adenocarcinoma is the main pathological diagnosis of this type of lung carcinoma. Although this cancer is usually a relatively lower grade malignancy with well or moderate tumor differentiation, early detection and surgical resection remain appropriate managment options.


 scan showed a round cavity in the upper lobe of the left lung with pure ground glass opacity (GGO). A: Coronal MSCT images showed diaphragmatic and pleural depressions, without an obvious burr sign (red arrow). B: A thin wall cavity was found in the left upper lobe of the lung with mixed GGO (red arrow). The CT scan showed that the inner wall of the cavity was smooth, and the wall thickness was uniform with multiple septal shadows.")
 scan showed an irregular cavity in the left upper lobe of the lung with spicule and vascular convergence signs. A: The CT scan showed that the lesion was located in the upper lobe of the left lung. The inner wall of the cavity was smooth, the thickness of the wall was not uniform, and internal septation was visible; the lesions were surrounded by ground glass opacity (GGO) and lobulated at the edge of the lesion (red arrow). B: The coronal view showed that the cavity was divided internally, blood vessels passed through the cavity, and the surrounding vessels were clustered (red arrow).")
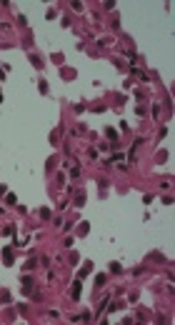
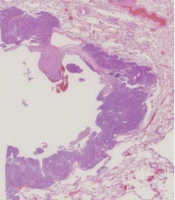
 staining showed lung adenocarcinoma, mainly distributed in the adenoid structure. Tumor cells grew along the alveolar wall in an adherent manner. The cell body was large, the nucleus was large and dark-stained, and the nucleus was irregular with nucleoli. B: A 60-year-old man with cough for one month undergoing surgery. Pathological examination demonstrated that the adenosquamous carcinoma tissue was distributed in nests, with a large cell body, an abundant cytoplasm, an eosinophilic, large, and deeply stained nucleus, and an irregular nuclear shape; in some areas, the tumor tissue had a glandular structure with heterotypic cells and infiltrative growth.")