




1. Background
Osteoid osteomas (OO) are the third most common benign bone tumors affecting mostly children and adolescents with more tendency toward males (1). Lower extremities, in particular femoral and tibia bones are the main area of involvement (1). OO is described by a characteristic pain that is intensified at nights and ascribed to the high level of prostaglandin formation in the affected area, leading to vasodilation and vascular proliferation which cause stimulation of peripheral nerve fibers. Therefore, non-steroidal anti-inflammatory drugs (NSAIDS) dramatically alleviate the pain (2). Other presenting signs that commensurate to the site of lesions include tenderness, swelling, limp, scoliosis, and bone deformity.
Main imaging modalities including plain radiographs, computed tomography (CT) scan, magnetic resonance imaging (MRI), and whole body bone scan (WBBS) along with clinical findings lead to the accurate diagnosis in most cases. The most common feature of OO is a small, well-delineated, low-attenuation nidus surrounded by a dense sclerotic reaction (3). Treatment options include medical therapy, surgical removal, and minimal invasive procedures such as CT or MRI-guided core drill excision, and percutaneous thermal ablation (PTA). Taking into consideration that conservative approaches take 6 to 15 years for symptom resolution as well as adverse effects of long term use of NSAIDS, surgical excision is the treatment of choice (4). Significant PTA procedures that refer to radio-frequency ablation (RFA) and interstitial laser photocoagulation (ILP) have also been recently applied with high success rates (5-10).
2. Objectives
The goal was to assess the safety and outcomes of RFL and ILP in patients with OO as well as compare the efficacy of these two procedures.
3. Patients and Methods
3.1. Patients
Medical records of OO patients were retrospectively reviewed. Diagnosis of OO was made based on clinical and imaging features. The patients were referred by orthopedic surgeons from the hospital clinic. Imaging methods used for diagnosis were plain radiography, CT scans and radio isotope bone scans. Written informed consent was obtained from all patients or their parents after detailed explanation of the procedure and the Ethics Committee of the University Research Deputy approved the study. All patients were followed up clinically either through outpatient clinic visit or telephone interview and imaging was conducted in case of reappearance of signs and symptoms of OO.
3.2. CT-Guided Radiofrequency Ablation
Our institutional review board approved this study. Informed consent was applied from the patients or their parents. One experienced interventional radiologist performed all RFA procedures in our university affiliated hospital on an inpatient basis.
All RFA procedures were done under general anesthesia and fluoroscopic CT guidance (Somatom, Siemens, Germany) with a thickness of 1 - 5 mm to localize the lesions. After prep and drep, under CT guidance we adjusted the position of the patient’s lesion and access into the nidus was made by a coaxial bone biopsy system. The tumor was ablated using a temperature of 60°C - 90°C for 3 - 7 min by 3 - 20 W power.
Postprocedural CT was done to rule out soft tissue swelling and hematoma. Patients were advised to avoid vigorous exercise and sports for 6 weeks.
Technique success of RFA was defined as placement of the tip of the electrode within the center of the nidus. Clinical success was defined as pain relief after treatment. Visual analogue scale was evaluated before and after treatment. Recurrence was defined as residual occurrence or reappearance of symptoms similar to those that manifested upon presentation.
3.3. CT-Guided Laser Photocoagulation
All procedures were carried out under general anesthesia. Under CT scan (Siemens, Germany) we localized the lesion and the dimensions of the nidus were measured.
We used Nd-YAG laser equipment with two watts power. An eight hundred micron fiber was inserted through the needle and the needle was withdrawn about 5mm to let the bare tip of the needle to remain within the tumor. Fiber precharing was done clinically by firing of fiber in a few milliliter of patient’s blood immediately before initiating the procedure.
3.4. Data Analysis
SPSS for Windows version 16 (SPSS Inc., Chicago, Illinois) statistical software was used for data analysis. Clinical success rates of RFA and ILP were compared, using chi-squared test. The odds ratios were calculated with 95% confidence intervals. Statistical significance was set at P value < 0.05.
4. Results
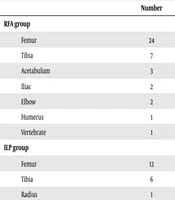
Sixty patients were included in this study. Characteristics of the patients are summarized in Table 1. Location of the lesions is shown in Table 2.
Table 1.Characteristics of Osteoid Osteoma Patients Treated with RFA and ILP
| RFA group (n = 40) | ILP group (n = 20) | |
|---|---|---|
| Age | ||
| Range | 3 - 42 | 5 - 79 |
| Mean | 18.02 | 19.30 |
| SD | 10.49 | 16.45 |
| Sex | ||
| Female | 12 | 5 |
| Male | 28 | 15 |
Abbreviations: ILP, interstitial laser photocoagulation; RFA, radiofrequency ablation; SD, standard deviation.
Table 2.Distribution of OO Lesions Based on the Anatomic Location
| Number | |
|---|---|
| RFA group | |
| Femur | 24 |
| Tibia | 7 |
| Acetabulum | 3 |
| Iliac | 2 |
| Elbow | 2 |
| Humerus | 1 |
| Vertebra | 1 |
| ILP group | |
| Femur | 13 |
| Tibia | 6 |
| Radius | 1 |
Abbreviations: RFA, radiofrequency ablation; OO, osteoid osteoma.
4.1. RFA
Forty patients underwent RFA. Patients were followed up from 4.5 to 16 months (mean = 10 and SD = 3.99). Forty one RFAs were performed. Pain relief was documented within 1 - 7 days in 35 and 1 - 3 months in five of the patients. The technical success rate was 100%. Recurrence of tumor occurred in four patients. Of these, one patient was successfully treated with the second RFA and open surgical excision was performed in two cases. Two fractures also occurred in two cases in the right iliac and left humorous bones that were both managed by nonsurgical methods. Therefore, the primary and secondary clinical effectiveness was 90.00% and 92.50%, respectively. The procedure was not complete in one patient who had OO of the pedicle of the fifth thoracic vertebrate to prevent spinal injury.
4.2. ILP
We performed 20 ILPs in 20 patients. The mean follow up time was 10.85 months (range = 2 – 16 and standard deviation [SD] = 3.49). Total pain relief was recorded within 1 - 7 days in 17 patients and within 3 months in one patient. Two patients had partial relief. The technical success rate was 100%. Initial clinical success rate was 85.00%.Three cases had recurrence. Of these, one patient was successfully retreated with ILP. Surgery was performed in two patients. Finally, the secondary success rate was 90.00%.
In comparison between the outcomes of RFA and ILP, no statistically significant difference was seen (P value > 0.05). In addition, as we mentioned, except for two cases of fractures, no other major complications happened in the two groups.
5. Discussion
Osteoid osteoma (OO) is a small, benign bone tumor that causes typical pain that often gets worse at night and is relieved by NSAIDs (1). OO has a distinctive feature that makes its diagnosis straightforward and is mainly diagnosed based on the presenting signs and symptoms and radiological findings. Characteristic radiographic findings include a nidus of vascular osteoid tissue in the bone cortex surrounded by reactive sclerotic bone (3). However, there may be lesions that mimic the imaging features of OO including Brodie abscess of chronic osteomyelitis with a radiolucent center and surrounding reactive sclerosis, chondroblastomas that occur in the epiphyses of children, osteoblastoma, stress fracture, osteomyelitis, eosinophilic granuloma, bone cyst, avulsion fracture, chondroblastoma, and intracortical hemangioma (11, 12). CT is the modality of choice for diagnosis of this tumor and provides the characterization of the nidus and the surrounding sclerotic bone. In addition, MRI and radionuclide scintigraphy are useful for detecting lesions (11, 13-15).
Surgical excision of the nidus is the treatment of choice; however, it has disadvantages such as difficulty locating the lesion intraoperatively, prolonged period of hospitalization and restricted activities, and postoperative complications (16, 17). Moreover, the location of some lesions may prevent surgical excision because of possible adjacent structure damage. Articular and epiphyseal lesion excision requires arthrotomy impairing bone growth and joint mobility.
Minimally invasive techniques have been developed over the recent decades that treat OO with less bone removal, shorter hospital stays and recovery, earlier resuming of daily activities, decreased morbidity, and recurrence rate compared to surgery (12). Percutaneous resection, ethanol injection, laser photocoagulation, and RFA have showed high success rates with low complications for the treatment of OO (5, 12, 18). Percutaneous laser photocoagulation uses optic fibers to achieve ablation of the nidus by producing thermal injury of the lesion rather than destruction through optical injury (13). Results of interstitial laser photocoagulation (ILP) and percutaneous radiofrequency coagulation (RFC) of osteoid osteoma are comparable, but expensive equipment is needed for ILP (13). The advantage of laser photocoagulation over radiofrequency ablation is that the access route for the laser fibre is smaller than for the radiofrequency electrode which minimizes damage, and it may allow earlier return to vigorous activity. Radiofrequency ablation may also be cheaper than laser photocoagulation.
In this cohort of patients, no histological confirmation was required since a dynamic-contrast CT was obtained in all patients.
In this study we evaluated the safety and efficacy of PTA procedures including RFA and ILP. Our data showed high success rates for both RFA and interstitial laser ablation (ILA) similar to previous published studies. Total pain relief occurred in 96.6% of the patients. As we mentioned, our major complication was fracture that occurred in two patients. In other studies, fracture has been rare and it has been reported as case report (19). Comparison of the two methods has shown similar results in previous studies. For example, in a clinical study conducted by Gebauer et al. (20) on thermal ablation of OO using laser interstitial thermal therapy on 12 patients and RFA in eight patients, pain relief ocurred in all patients after the first ablation. Recurrence occurred in three patients after 3, 9, and 10 months that was successfully re-treated. No major complications were reported. It was concluded that thermal ablation is a safe method for OO. In addition, they reached the conclusion that there is no difference in the clinical outcome between the two methods (20). It has been mentioned that RFA and open surgery have similar treatment outcomes; however, RFA is preferred as it has a shorter hospital stay and recovery period (21). Some studies have reported a clinical efficacy of 100% for RFA (21). An advantage of RFA under the guidance of CT is the rapid frame rate and highly resolved visualization of bony structures. These characteristics allow the interventionist to perform the procedure in a real-time manner (22). Comparing the cost of the two methods, as we mentioned, laser ablation device is more expensive, but performing each procedure by RFA needs a more expensive probe compared to laser ablation. Average total costs per patient is higher in RFA compared to laser ablation (about 20% higher in RFA compared to laser) (22). Needle navigation could be performed by ultrasongraphy, CT, fluoroscopy and MRI. As OO is not very detectable in ultrasonography, it is not the method of choice. CT fluroscopy guidance is better due to its real time control possibility (21).
There are limitations in this study. The retrospective nature of this study and data collection is the major limitation. Because of the retrospective nature of the study, we did not have access to the important missing data. In addition, lack of a control group treated by surgery made a definite comparison with surgery difficult. The small sample size was another limitation.
In conclusion, similar to previous published studies, this study showed high success rates for both RFA and ILA.

