





1. Background
Every year, more than 200 million adults undergo surgery worldwide, and the number of these patients is increasing (1). In Iran, according to the statistics of the Ministry of Health and Medicine, an average of 1 million and 5 hundred thousand major surgeries are performed annually (2). Studies have shown that 36.57% of patients undergoing surgery experience at least one of the complications in the postoperative period, and approximately 20% of all patients undergoing abdominal surgery experience fever complications in the postoperative period (3). According to the classification of the World Health Organization, about 10% of patients who have undergone surgery experience complications, such as cyanosis and fluctuations in the arterial blood oxygen saturation percentage (3, 4).
Among the complications after surgery, we can mention changes in temperature and drop in oxygen saturation of arterial blood (5). Fever is one of the causes of increased length of stay and readmission to the hospital, which causes concern for the care team and the patient. Diagnosing and differentiating postoperative fever from acute infection is of particular importance for the treatment team because this fever can have adverse effects in the treatment process (6). However, in surgeries performed on the abdomen and chest, this complication is obvious and can cause a decrease in vital capacity and the occurrence of atelectasis and pneumonia (5). Managing postoperative complications and reducing their incidence is one of the necessities of nursing care in the postoperative phase (7). It is emphasized to identify and use new therapeutic interventions that can be used more effectively, less expensively, and more effectively while affecting vital signs and complications with greater safety. Especially in major surgeries where patients face more complications, the use of these methods, along with the usual methods, can play an effective role in helping patients achieve health and recovery and reduce costs for health systems (8, 9).
One of the non-medicinal methods is massage, which is a short-term care measure in the form of manipulation of the soft tissue of the body and can have different effects on the mental state, anxiety, and physiological variables (10). Massage releases endorphins reduces many symptoms related to pain and inflammation, and makes a person feel comfortable. The massage method can be easily performed by the care team members, patients themselves, or their family members by spending the least possible time. Also, if the patient does not have a specific lesion or underlying disease, these methods usually do not cause any complications; thus, they are considered a safe method to improve the symptoms of patients (11).
In addition to various studies in the field of non-pharmacological methods conducted on various physiological indicators, what is still a challenge in these studies is that different non-pharmacological methods, including massage, can create a variety of effects (11). Also, this point is still questionable whether the effectiveness of these methods is different based on the severity of the physiological symptoms caused by the disease in the investigated groups or whether the nature and type of the technique used have led to a different spectrum of their effectiveness (12-14). It should also be noted that the results of various methods (such as massage), in addition to being uncomplicated, can be used as a reliable method along with other treatment methods to reduce the complications of different groups of patients (15, 16).
Despite the existence of various studies on the effect of massage on patients, there were few studies on the effect of this method on body temperature and arterial blood oxygen saturation in patients undergoing surgery. Azimian et al. conducted a study on the effect of foot massage on the level of consciousness of comatose patients, showing that massage can significantly increase the level of consciousness of these patients (12). Kardan et al. stated that foot reflexology massage could have a significant effect on physiological indicators, as well as pain and fatigue in coronary angiography patients (13). Further, YekeFallah et al. conducted a study on the effect of hand touch on the vital signs of concussion patients hospitalized in the intensive care unit (ICU), indicating that massage can be effective on blood pressure but not on temperature (14).
Song et al. investigated the effect of self-reflexology massage on the improvement of vital signs in healthy people, showing that foot reflexology did not improve blood pressure (17). Further, Khoshtarash et al. showed the effect of foot reflexology massage on pain after cesarean section, but this method did not have a significant effect on the physiological indicators of patients (15). Sayari et al. also found that the massage method was effective in the blood oxygen saturation of patients with infarction but not in the heart rhythm and other vital signs (16). Azami et al. also reported a significant short-term effect of foot massage on arterial blood oxygen saturation in neurosurgery patients admitted to the ICU (18).
In the analysis of the above results, it should be said that different studies have expressed the effect of various massage methods on different organs on hemodynamic indicators. Also, the effect of these methods has been investigated in different patients. What is discussed as a gap between studies in this field is that, first, the results of the effect of massage on vital indicators have been expressed differently in studies, and significant and non-significant effects have been reported in different groups of patients. Second, there were few studies on the effect of local massage on blood oxygen saturation and body temperature, especially in patients undergoing thoracic and abdominal surgery.
2. Objectives
The present study was designed and implemented to investigate the effect of the local massage method on body temperature and blood oxygen saturation percentage of this group of patients.
3. Methods
3.1. Study Design
This research is a semi-experimental study with 2 groups and before and after design, which was conducted in Shahrekord city in 2019. The research population included all patients who underwent thoracic and abdominal surgery in Kashani Shahrekord Hospital.
3.2. Sampling Method
Sampling was done by the convenience method. The sample size according to the formula in interventional studies
3.3. Randomization
After entering the study, the patients were divided into 4 blocks using the 2 variables of surgery type and doctor type using the block classification randomization method. First, based on the information of the patients, the researcher determined the eligibility of the patient to enter the study and which block each patient belongs to (doctor type). Then, from 4 sheets (which included 2 numbers A (massage) and 2 numbers B (control) in 1 envelope), we presented the envelope to the patient and asked them to remove a sheet from the envelope. Then, based on the removed sheet, she was placed in the relevant group, and this process continued for each patient until the block of 4 was completed. After completing 1 block, the next block was also completed with the same algorithm.
3.4. Intervention
To conduct this research, after obtaining the necessary permits from the competent centers of the university and presenting them to Kashani Shahrekord Educational and Treatment Center, the study method and its objectives were first explained to the patients and their companions, and if they wish to participate in this research, written consent was obtained from the patient or the patient's legal guardian. The demographic information form of the patients was completed by the researcher. Before the interventions, arterial blood oxygen saturation was measured using a wired digital pulse oximetry device (SA model), and the temperature was monitored using a Beurer contact thermometer (Germany), which was controlled and calibrated by the researcher before use. After the patients were awake, temperature changes and arterial blood oxygen saturation were measured and recorded by the researcher. In the intervention group, in addition to routine care, the surface massage of hands and feet from finger to wrist (individual fingers, soles, and backs of hands, feet, and wrists) was performed in four 5-minute intervals for each part of the patient and for a total of 20 minutes. This intervention was performed 3 times a day for 48 hours for these patients. During all this time, the researcher was present at the patient's bedside and provided care only regarding the intervention. The steps of the massage were as follows: First, the base of each finger was held between the thumb and other fingers, and it was stretched along each finger to its tip and rotated outward.
The patient's toes were stretched along each toe and then bent forward and backward while stretching. The soles of the patient's feet were rubbed with the thumb from the heel to the ridge under the toes. While the patient's foot was on the upper side, using the thumb or other fingers, pressure was slowly applied between the tendons of the wrist and the fingers (19). First, the right foot was massaged, followed by the left foot, right hand, and left hand. For the massage, a masseur of the same gender as the patient was used, and their agreement coefficient was previously measured (91%). After the intervention, temperature changes and arterial blood oxygen saturation were again evaluated by the researcher. The control group only received routine care according to the treatment protocol, and no intervention was performed by the researcher; after 48 hours, the researcher completed the questionnaire again with questions from the patient.
3.5. Statistical Analysis
The investigation of normal distribution for quantitative variables was performed using the Kolmogorov-Smirnov test. The obtained data were analyzed using SPSS version 16 (SPSS Inc, Chicago, IL, USA), descriptive statistical tests (prevalence, frequency percentage, and mean and SD), and inferential statistical tests (paired t-test, t-test, analysis of variance (ANOVA), and chi-square test).
4. Results
The results of the Kolmogorov-Smirnov test indicated that the study variables were normal (P > 0.05). Analysis of variance and chi-square tests showed that the demographic variables were not significantly different in the 2 groups (P > 0.05). The distribution of research units in terms of demographic variables is shown in Table 1.
Table 1.The Frequency of Demographic Characteristics of Patients Undergoing Surgery According to Different Massage and Control Groups (n = 60)
| Demographic Characteristics | Intervention (Massage), No. (%) | Control, No. (%) | Test |
|---|---|---|---|
| Age | P = 0.208; F = 1.427 | ||
| 18 - 25 | 3 (10) | 1 (3.3) | |
| 26 - 35 | 6 (20) | 2 (6.6) | |
| 36 - 45 | 6 (20) | 3 (9.9) | |
| 46 - 55 | 9 (30) | 11 (36.6) | |
| > 56 | 6 (20) | 13 (43.3) | |
| Total | 30 (100) | 30 (100) | |
| Sex | P = 0.727; χ2 = 1.23 | ||
| Male | 17 (56.7) | 16 (56.3) | |
| Female | 13 (43.3) | 14 (44.7) | |
| Type of doctor | P = 1; χ2 = 1.005 | ||
| 1 | 12 (40) | 13 (43.3) | |
| 2 | 9 (30) | 8 (26.6) | |
| 3 | 5 (16.7) | 5 (16.7) | |
| 4 | 4 (13.3) | 4 (13.3) | |
| Type of surgery | P = 0.98; χ2 = 0.54 | ||
| Abdomen | 23 (76.7) | 23 (76.7) | |
| Chest | 27 (23.3) | 27 (23.3) | |
| Type of anesthesia | P = 0.533; χ2 = 2.11 | ||
| General | 28 (93.3) | 28 (93.3) | |
| Spinal | 2 (6.7) | 2 (6.7) |
The result of the t-test showed that the average arterial blood oxygen saturation in the research units before the intervention was not significant according to different groups (P = 0.95). Also, the average arterial blood oxygen saturation between different massage and control groups was not significant after the intervention (P = 0.52). The average temperature in the research units before the intervention according to different groups (P = 0.303) and after the intervention according to different groups (P = 0.38) was not significant. The paired t-test also indicated that the oxygen saturation in the massage group increased significantly after the intervention compared to before (P < 0.001). Also, body temperature changes were significant in the massage group after the intervention compared to before (P = 0.005; Table 2).
Table 2.Comparison of Mean Arterial Blood Oxygen Saturation and Body Temperature Between the Massage and Control Groups Before and After the Intervention (n = 60) a
| Variables | Massage | Control | t-Test |
|---|---|---|---|
| SpO2 (%) | |||
| Before | 89.5 ± 6.7 | 89 ± 4 | P = 0.95; T = 4.55 |
| After | 92.4 ± 5.5 | 91 ± 4.8 | P = 0.52; T = 1.134 |
| Paired t-test | P < 0.001; T = 1.162 | P < 0.001; T = 3.176 | - |
| Body temperature (°C) | |||
| Before | 37.3 ± 3.3 | 37.3 ± 0.3 | P = 0.303; T = 5.54 |
| After | 37 ± 1.2 | 37.2 ± 0.3 | P = 0.38; t = 4.096 |
| Paired t-test | P = 0.019; T = 2.003 | P = 0.36; T = 2.304 | - |
a Values are expressed as mean ± SD unless otherwise indicated.
5. Discussion
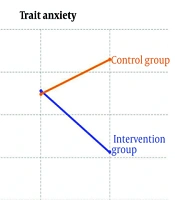
The aim of this study was to determine the effect of local massage on arterial blood oxygen saturation and body temperature of patients undergoing thoracic and abdominal surgery. The results showed that massage significantly improved the percentage of patients' peripheral oxygen saturation (SpO2) and body temperature after the operation compared to before; however, these changes were not significant compared to the control group.
Abdi et al. investigated the effect of foot massage on the blood pressure and pulse of patients admitted to the ICU, showing that massage results in a significant change in the blood pressure and pulse of these patients (21). Sayari et al. conducted a study on the effect of foot massage on the physiological indicators of patients suffering from acute myocardial infarction, showing that massage is effective in oxygen saturation of these patients but is not effective in other physiological indicators (blood pressure and pulse), temperature, and heart rate (16).
Zhang et al. investigated the effect of massage on patients with cold tolerance disorder, showing that foot reflexology massage increases the temperature of the foot and skin in the massage area (22). Lee investigated the effect of foot massage on skin temperature, indicating that this massage can increase skin temperature (23). In the study by Sayari et al, foot massage did not show a significant effect on body temperature in patients with heart infarction (16). YekeFallah et al. investigated the effect of hand massage on vital signs in concussion patients admitted to the ICU, showing that massage has a significant effect on the breathing and blood pressure of patients; however, it did not have a significant effect on the temperature of these patients (14).
Rafati et al. investigated the effect of massage on the physiological responses after pain caused by blood sampling in infants, indicating that there is a significant difference in the intensity of pain, heart rate, breathing, and duration of the infant's cry. They concluded that massage had a positive effect on reducing some physiological responses (such as pain) caused by blood collection in infants (24). Taghizadeh et al. investigated the effects of stroke massage and reflexology massage on physiological indicators in patients suffering from heart attack, showing the positive effects of stroke massage on temperature and arterial blood oxygen saturation, as well as reflexology massage on pulse and temperature (25). Kardan et al. investigated the effect of foot reflexology massage on fatigue, pain, and physiological indicators of patients after coronary angiography, showing that foot reflexology massage affects fatigue, pain, and physiological indicators of systolic and diastolic blood pressures after coronary angiography (13). Azami et al. investigated the effect of short-term foot massage on arterial blood oxygen saturation values, showing a significant increase in arterial blood oxygen saturation. It can be said that following the foot massage, there are changes in the metabolism, as a result of which the consumption of oxygen decreases, and its values increase after the massage (18).
Song et al. investigated the effect of self-reflexology massage on the improvement of vital signs in healthy people, showing that foot reflexology did not improve blood pressure (17). Khoshtarash et al. investigated the effect of foot reflexology massage on pain after cesarean section and showed that this method did not have a significant effect on the physiological indicators of patients (15). Wilkinson et al. conducted a study on the effect of reflexology massage on patients with chronic obstructive pulmonary disease; the results did not show a significant effect on the percentage of arterial blood oxygen saturation (26). Mohammadpour et al. also did not report significant results in their study regarding the effect of massage on physiological indicators (27).
It is important to note that various studies have reported both the effects and lack of effects of massage on different physiological variables. Regarding the effect of massage on vital variables (such as arterial blood oxygen saturation and temperature), it is worth mentioning that the massage method can reduce anxiety and stress in patients by creating a state of relaxation and releasing endorphins; therefore, it could positively affect vital variables. The differences in the results may be due to the nature of massage itself. The massage itself includes different methods and is performed by different people in terms of depth, intensity, and time.
5.1. Conclusions
There was a significant difference in arterial blood oxygen saturation and body temperature compared to before the intervention, but these changes were not significant compared to the control group. Massage, as complementary medicine, can have positive effects on patients undergoing surgery; therefore, it should be considered by care team members. In this regard, it is recommended to consider various types of complementary medicine (including massage) in in-service training programs. In addition to being cost-effective, massage does not have any serious complications and drug interactions in almost all cases; it is also easy to perform and accepted by the patient. Further, complementary medicine can be used to reduce anxiety and maintain hemodynamic balance. More studies are needed to further investigate the impact of this method on the vital variables of patients after surgery. Regarding the limitations of the present study, the use of the available non-random sampling method should be mentioned; however, we tried to control this limitation with the random allocation method. In addition, blinding was not possible in this study.