







1. Background
Currently, the diagnosis of COVID-19 primarily relies on polymerase chain reaction (PCR) tests (1). Computed tomography (CT) findings often resemble those seen in other viral infections, notably peripheral patchy ground-glass opacities (GGOs) and consolidations (2). Despite the low diagnostic specificity of these features, CT can provide an objective assessment of disease severity, serving as a radiologic marker for overall disease burden (3). The CT is the preferred imaging modality for evaluating the lung parenchyma (4). Several CT grading systems have been developed to assess the extent of lung involvement in COVID-19 patients. Among these, the CT total severity score (TSS) has been shown to offer the highest specificity and greatest time efficiency compared to other scoring systems (5).
Even though the primary focus has been on pulmonary manifestations, clinicians should remain aware of the potential impact of COVID-19 on other organs. Critically ill patients are at risk of developing acute kidney injury (AKI) — defined as increased serum creatinine (SCr) and decreased urinary output — which is associated with poorer outcomes (6). In fact, there is strong evidence linking AKI, alongside respiratory complications in COVID-19 patients, to worse prognoses, with some studies reporting mortality rates as high as 35% (7). Beyond direct viral injury to renal cells, secondary effects such as systemic inflammation, hypoperfusion, rhabdomyolysis, and thromboembolic events may also contribute to kidney injury during the course of the disease. Furthermore, the possibility of a kidney-lung crosstalk mechanism should not be overlooked. This hypothesis suggests that lung injury-induced activation of inflammatory cytokines, particularly IL-6, increases alveolar capillary permeability, leading to alveolar hemorrhage and systemic organ dysfunction, including kidney damage (8). Microvascular injury to the kidney may thus be a consequence of this systemic inflammatory response (9).
2. Methods
2.1. Patients
This cross-sectional study included 50 patients admitted to Afzalipour Hospital, Kerman, Iran, between April and September 2020. Consecutive sampling was employed for the inclusion of participants. All patients had confirmed COVID-19 infection by PCR during hospitalization. Non-contrast chest CT scans were performed on all patients. Individuals with pre-existing malignancies, chronic pulmonary diseases, or prior renal impairment were excluded from the study to eliminate potential confounding factors. The AKI was defined based on the following criteria: An increase in SCr of ≥ 0.3 mg/dL within 48 hours, or ≥ 1.5 times the baseline level over 7 days. A urine output of < 0.5 mL/kg/hour for at least 6 hours was also classified as AKI (10). The study adhered to the ethical guidelines outlined in the Helsinki Declaration (11) and was approved by the Ethics Committee of Kerman University of Medical Sciences (IR.KMU.REC.1401.112).
2.2. Laboratory Data
Laboratory data were extracted from the hospital’s health information system (HIS) and included the following parameters: (1) SCr, (2) serum sodium, (3) serum potassium, and (4) urinary output. The normal ranges for the above indices were as follows:
(1) SCr: 0.7 to 1.3 mg/dL.
(2) Serum sodium: 135 to 145 mEq/L.
(3) Serum potassium: 3.5 to 5.2 mEq/L.
(4) Urinary output: 800 to 2,000 milliliters per day.
(5) Estimated glomerular filtration rates (eGFR): > 90.
All mentioned indices were measured once daily according to hospital protocol. Glomerular filtration rate (GFR) was calculated using the MDRD formula (12). Changes in sodium and potassium levels from admission to discharge were also documented. Data were recorded on custom-designed charts by the research team. Subsequently, the recorded data were cross-checked by another researcher to verify consistency, accuracy, and compliance.
2.3. Computed Tomography Acquisition
Chest CT images were acquired using a 64-slice CT scanner (Siemens Medical System Inc., Erlangen, Germany). Scans were performed at the time of admission with the patient in the supine position during inspiration, and in a caudocranial direction. All scans fully covered the lung parenchyma, from the lung apices to the diaphragm. Images not meeting these criteria, as well as those with significant imaging artifacts, were excluded. No contrast medium was used. The standard CT acquisition protocol included a tube voltage of < 120 kVp, automated tube current adjustment, and a low-dose CTDIvol of < 3 mGy. Scout images were obtained from the base of the neck to the uppermost portion of the kidneys.
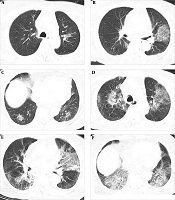
Two expert radiologists, with 10 and 4 years of experience respectively, independently reviewed the images using the INFINITT PACS system (INFINITT Healthcare Co. Ltd., Seoul, South Korea). The radiologists were blinded to the patients’ laboratory data. All images were interpreted in the standard mediastinal view across axial, coronal, and sagittal planes. To evaluate the extent of pulmonary involvement, a TSS was calculated based on the presence of GGOs, consolidation, or mixed GGO in each lobe (Figure 1). Each lobe was scored from 0 to 4: Zero (no involvement), 1 (1 - 25% involvement), 2 (26 - 50%), 3 (51 - 75%), and 4 (> 75% involvement). The sum of scores from all lobes was used to calculate each patient’s TSS, ranging from 0 to 20 (5). Each 4-point increment in TSS was considered one unit of lung involvement severity (13).

Figure 1.
Pulmonary involvement in a patient with COVID-19
Axial CT scan of a 43-year-old male with confirmed COVID-19. As indicated by the arrows, multiple bilateral GGOs are visualized in the pulmonary fields. The TSS was calculated by summing the involvement scores of all five pulmonary lobes.
2.4. Statistical Analysis
Data were analyzed using SPSS software (version 26), with statistical significance set at P < 0.05. Cases with missing data were initially excluded from the analysis. Quantitative data were reported as numbers and percentages. Correlations between variables were assessed using Spearman’s correlation test. Multiple linear and logistic regression models were employed to determine the association between TSS and other variables.
3. Results
Of the 50 included participants, 23 were male (N = 23, 46%), and the mean age was 46.88 ± 16.23 years. The demographic and clinical characteristics of the participants are presented in Table 1. No significant correlation was detected between TSS and gender, age, or changes in serum sodium and potassium levels. A strong positive correlation was observed between the severity of lung involvement on CT scans and SCr levels (P < 0.0001), as well as GFR (P = 0.022) (Tables 2 and 3). An independent t-test revealed a significant association between TSS and the presence of AKI, as well as reduced urinary output (P < 0.001) (Table 3) The logistic regression model demonstrated that an increase of one unit in the severity of lung involvement significantly increased the odds of AKI by 5.099 times (P = 0.031), and the odds of reduced urine output by 14.040 times (P = 0.026) (Table 4).
Table 1.Demographic and Clinical Characteristics of the Participants
| Variables | No. (%) or Mean ± SD | Range |
|---|---|---|
| Age (y) | 48.88 ± 16.23 | 22 - 79 |
| Gender (male) | 23 (46) | - |
| TSS | 18.36 ± 7.65 | 0 - 20 |
| Creatinine (mg/dL) | 2.06 ± 0.87 | 0.70 - 3.50 |
| Sodium (mEq/L) | 139.43 ± 6.21 | 131 - 149 |
| Potassium (mEq/L) | 4.41 ± 1.66 | 3.1 - 5.6 |
| GFR (mL/min) | 102 (9.71) | 82 - 115 |
| Urinary output (mL/day) | 1348 (324) | 680 - 1800 |
Abbreviation: GFR, glomerular filtration rate; TSS, total severity score.
Table 2.Correlation Between Severity of Pulmonary Involvement and Serum Creatinine, Glomerular Filtration Rate, Age, and Changes in Sodium and Potassium Levels
| Variables | Cr | GFR | Age | Changes in Na/K |
|---|---|---|---|---|
| Severity of lung involvement | ||||
| Correlation coefficient | 0.959 | -0.432 | 0.142 | 0.133/0.121 |
| P-value | < 0.0001 | 0.022 | 0.113 | 0.291/0.893 |
| N | 50 | |||
Abbreviation: GFR, glomerular filtration rate.
Table 3.Independent t-Test for Evaluation of the Relationship Between Total Severity Score and Gender and Presence of Acute Kidney Injury and Reduced Urinary Output
| Variables | N | Mean ± SD | df | P-Value |
|---|---|---|---|---|
| Gender | 39.96 | 0.842 | ||
| Female | 27 | 18.55 ± 6.15 | ||
| Male | 23 | 18.13 ± 8.31 | ||
| Presence of AKI | 48 | 0.001 | ||
| Yes | 29 | 21.43 ± 3.64 | ||
| No | 21 | 14.12 ± 4.32 | ||
| Presence of reduced urinary output | 48 | 0.001 | ||
| Yes | 25 | 22.81 ± 2.53 | ||
| No | 25 | 16.55 ± 3.27 |
Abbreviation: AKI, acute kidney injury.
Table 4.Logistic Regression Model to Show the Separate Relationship of Total Severity Score with Presence of Acute Kidney Injury and Reduced Urinary Output
| Variables | B | P-Value | OR | 95% CI for OR | |
|---|---|---|---|---|---|
| Lower | Upper | ||||
| Presence of AKI | 1.629 | 0.031 | 5.099 | 1.161 | 22.397 |
| Presence of reduced urinary output | 2.642 | 0.026 | 14.040 | 1.371 | 143.813 |
Abbreviation: AKI, acute kidney injury.
4. Discussion
To the best of our knowledge, this is the first study in Iran to evaluate lung parenchymal involvement in COVID-19 patients with AKI. In this study, we examined the association between the severity of lung involvement, as assessed by chest CT, and the incidence of AKI in COVID-19 patients during hospitalization.
The CT scans have been widely used to assess the extent of lung involvement in COVID-19, revealing characteristic features of lung lesions (10). The severity of lung involvement ranges from mild to severe, with more extensive lung damage associated with poorer clinical outcomes (14). The CT imaging is particularly valuable for the early detection and monitoring of disease progression, enabling clinicians to make informed decisions about patient management and treatment strategies (15). On the other hand, renal complications — particularly AKI — have emerged as significant concerns in hospitalized COVID-19 patients. The development of AKI in this population is influenced by several factors, including age, pre-existing comorbidities (e.g., hypertension, diabetes), abnormal immune responses, and the presence of multi-organ dysfunction (16).
Both lung involvement, as visualized on CT, and AKI are critical indicators of COVID-19 severity. Understanding the relationship between these two factors may offer insights into the systemic nature of the disease and guide treatment approaches. To assess lung involvement, we used a semi-quantitative scoring system previously applied by Li et al. (17). Our study aimed to determine whether the severity of lung involvement significantly increases the risk of kidney failure and reduced urine output. Our findings revealed that for every unit increase in lung involvement severity, the probability of developing AKI increased by 5.099 times, demonstrating a strong correlation between the extent of pulmonary damage on CT and the risk of kidney failure in COVID-19 patients. This underscores the systemic impact of COVID-19 and the role of severe lung involvement in contributing to organ dysfunction. Moreover, we observed that the severity of lung involvement increased the likelihood of a decline in urine output by 14.040 times. Monitoring urine output is essential, as it serves as a critical indicator of kidney function and fluid balance. A reduction in urine output may signal impaired kidney function and reflect the broader systemic effects of COVID-19. Our results align with those of Tharwat et al., who identified a higher TSS as a major risk factor for mortality in hospitalized COVID-19 patients (18). Similarly, another study found that patients with more severe pulmonary involvement had lower eGFR and higher mortality rates (19). These findings highlight the significant relationship between lung involvement, kidney function, and patient outcomes in COVID-19. Therefore, patients with a higher TSS may require closer hospital monitoring and care. A higher TSS appears to be a reliable index for assessing the risk of AKI in patients with COVID-19.
Interestingly, our study did not find a significant correlation between the severity of lung involvement and changes in electrolyte levels (sodium and potassium). However, previous research has demonstrated that electrolyte imbalances — such as hyponatremia, hypernatremia, and hyperkalemia — are associated with poor prognosis in COVID-19 patients, independent of renal function (20). This suggests that electrolyte disturbances in COVID-19 may reflect systemic effects that extend beyond renal impairment. It has been proposed that a substantial proportion of patients with mild to moderate COVID-19 may exhibit perfusion defects in both the lungs and kidneys, potentially indicating systemic microangiopathy with microthrombosis as a key mechanism of AKI. This could result from the inflammatory response triggered by lung involvement, which increases alveolar capillary permeability and leads to alveolar hemorrhage, potentially provoking systemic organ dysfunction, including AKI due to microendothelial disturbances. Furthermore, previous animal studies have reported elevated levels of angiotensin II in subjects with COVID-19, which may serve as a mediator of acute pulmonary injury (21, 22). Additionally, electrolyte imbalances in COVID-19 patients might be attributed to gastrointestinal losses, including diarrhea and vomiting (22). To the best of our knowledge, none of our patients developed gastrointestinal complications, which may explain why electrolyte imbalances were not as prominent in our cohort compared to other studies. Further large-scale prospective cohort studies are essential to confirm the relationship between electrolyte disturbances and the severity of lung involvement, and to establish their clinical relevance.
There were several limitations to our study. First, it was conducted at a single center, which may have introduced selection bias. Additionally, the retrospective study design inherently provides a lower level of evidence compared to prospective studies. One important variable that we were unable to include in our analysis was the time interval between symptom onset and CT acquisition, which may have influenced the TSS values. We recommend that future multicenter studies adopt a prospective approach with larger sample sizes and include additional variables such as liver function tests and lactate dehydrogenase (LDH), which could provide further insight into organ function and mortality outcomes. Furthermore, investigations aimed at exploring the underlying mechanisms of kidney-lung interaction would be valuable to validate our findings across diverse populations.
4.1. Conclusions
Overall, the severity of lung parenchymal involvement observed on CT images correlates with elevated SCr levels, reduced urinary output, and a higher incidence of AKI during hospitalization. The increased risk of AKI associated with greater lung involvement underscores the need for integrated and multidisciplinary approaches to patient care in COVID-19. Future research should investigate the underlying mechanisms of kidney-lung interactions and consider multicenter studies to validate these findings across diverse populations.