






1. Background
Chronic kidney infection leads to irreversible damage and the development of kidney failure (1). In clinical conditions of end-stage renal disease, a severe form of chronic kidney infection, alternative treatment methods such as hemodialysis (HD), peritoneal dialysis, and kidney transplantation are employed. Over 90% of patients at this stage benefit from HD treatments (2, 3). Hemodialysis treatments are more effective with intravascular access, including internal arteriovenous fistula, arteriovenous graft, or central venous catheter (4, 5). With advancements in blood purification technology, the use of central venous catheters has gained more attention. However, these catheters are associated with complications such as thrombosis, infection, stenosis, and dysfunction (6).
In recent years, advanced techniques have reduced exit-site and tunnel infections, but catheter-related bloodstream infections (CRBIs) remain a significant challenge. Failure to improve and maintain catheter effectiveness can lead to serious complications, including cardiovascular diseases, cerebrovascular disorders, and increased mortality (7). The incidence rate of this infection is estimated to be approximately 1.2 - 2.5 per 1,000 patient-days (8, 9). This rate is reported to be higher in developed countries such as the United States and Canada compared to middle-income countries and India (10, 11). The CRBI is associated with significant mortality and hospitalization rates, with a mortality rate over three times higher than other bloodstream infections (12).
Previous studies have identified underlying diseases, catheter usage type, personal hygiene practices by patients and healthcare staff, recent hospitalization or surgery, and inadequate sterilization as potential risk factors for CRBI (13, 14). Additionally, gram-positive bacteria, including Staphylococcus aureus and methicillin-resistant S. aureus, with a prevalence of 80% in the community, are the most common microorganisms associated with CRBI (15-17).
2. Objectives
Despite stringent aseptic techniques, CRBI continues to occur at unacceptable rates. Considering the role of central venous catheter use in increasing bloodstream infections and length of hospital stay in HD patients (18, 19), the present study aimed to investigate the epidemiology of CRBI, associated factors, mortality rate, and factors associated with mortality in patients with this infection at Velayat Hospital in Qazvin province from 2018 to 2022.
3. Methods
This cross-sectional descriptive-analytical study included 592 patients with CRBIs treated in the HD unit of Velayat Hospital in Qazvin province between 2018 and 2022. Velayat Hospital is a referral center for chronic kidney disease treatment in Qazvin province, located in the northwest of the country, 135 kilometers from Tehran, providing public healthcare services. On average, approximately 97 patients with catheter infections are admitted and treated at this hospital annually. We extracted demographic and clinical information of patients with catheter infections admitted to this unit during the specified period. The data collected included age, gender, length of stay, time interval from admission to infection, catheter insertion site, type of identified organism, culture sample, hospitalization outcome, and antibiotic resistance status. Medical records with incomplete information were excluded from the study.
3.1. Data Analysis
Data analysis was performed using SPSS version 26 software. Quantitative data were described using means and standard deviations, while qualitative data were presented as frequencies and percentages. In this study, in addition to examining the prevalence of catheter infections based on various demographic and clinical variables, the relationship between different variables and patient outcomes (recovery or death) was also analyzed. For this purpose, logistic regression analysis was employed. After conducting univariate logistic regression analysis, multivariate logistic regression analysis was used to adjust for the effects of confounding variables. The level of statistical significance for all analyses was set at P ≤ 0.05.
4. Results
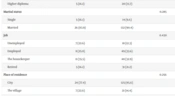
Data were collected from 592 patients with catheter infections, comprising 261 (44%) males and 331 (56%) females. According to the descriptive results, most individuals (277 patients; 47.6%) were in the age range of 60 - 79 years. The most common catheter insertion site was the cervical vein (270 patients; 46.9%). Regarding the types of microorganisms, S. aureus and Escherichia coli were the most prevalent catheter-related microorganisms, with 239 (41.4%) and 65 (11.2%) cases, respectively. The mortality rate due to catheter infection among patients was 19.6%. Other clinical information on patients is presented in Table 1.
Table 1.Demographic and Clinical Information of the Patients with Catheter Infections (2018 - 2022), Stratified by Gender (N = 592)
| Variables | Total | Male | Female |
|---|---|---|---|
| Age | |||
| ≤ 19 | 12 (2.1) | 6 (2.3) | 6 (1.9) |
| 20 - 39 | 66 (11.3) | 23 (8.8) | 43 (13.4) |
| 40 - 59 | 181 (31.1) | 86 (33.0) | 95 (29.6) |
| 60 - 79 | 277 (47.6) | 123 (47.1) | 154 (48.0) |
| 80 ≤ | 46 (7.9) | 23 (8.8) | 23 (7.2) |
| Catheters place | |||
| Jugular vein | 270 (46.9) | 131 (50.2) | 139 (43.3) |
| Femoral | 256 (44.0) | 107 (41.0) | 149 (46.4) |
| Others | 56 (9.6) | 23 (8.8) | 33 (10.3) |
| Organisms | |||
| Acinetobacter | 56 (9.6) | 26 (10.0) | 30 (9.3) |
| Staphylococcus | 239 (41.1) | 108 (41.4) | 131 (40.8) |
| Stenotrophomonas | 32 (5.5) | 19 (7.3) | 13 (4.0) |
| Escherichia coli | 65 (11.2) | 28 (10.7) | 37 (11.5) |
| Enterococcus | 26 (4.5) | 7 (2.7) | 19 (5.9) |
| Pseudomonas | 58 (10.0) | 32 (12.1) | 26 (10.0) |
| Klebsiella | 57 (9.8) | 28 (10.7) | 29 (9.0) |
| Enterobacter | 24 (4.1) | 10 (3.8) | 14 (4.4) |
| Others | 26 (4.2) | 9 (3.4) | 15 (5.1) |
| Result | |||
| Recovery | 456 (80.4) | 203 (80.6) | 253 (80.3) |
| Death | 111 (19.6) | 49 (19.4) | 62 (19.7) |
| Sample type | |||
| Shaldon | 302 (52.2) | 129 (49.8) | 173 (54.1) |
| Blood | 272 (47.0) | 127 (49.0) | 145 (45.3) |
| Others | 5 (0.9) | 3 (1.2) | 2 (0.6) |
| Length of stay | 18.04 (12.27) | 18.13 (12.40) | 17.97 (12.18) |
| Time from hospitalization to infection | 11.41 (10.06) | 11.54 (10.49) | 11.30 (9.70) |
| Time from catheter placement to infection | 29.84 (33.87) | 29.07 (32.19) | 30.46 (35.23) |
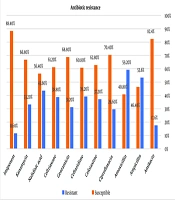
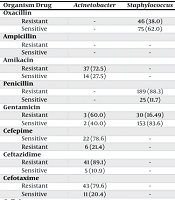
Regarding the antibiotic resistance of microorganisms in patients with catheter infections, the highest resistance rates were reported for Staphylococcus against penicillin (PEN) and clindamycin (CLU), at 88.3% and 56.9%, respectively. The lowest rates of antibiotic resistance were observed in E. coli against ampicillin (AMP), gentamicin (GEN), and chloramphenicol (CAM). Detailed resistance rates are presented in Table 2.
Table 2.Antibiotic Resistance Rates of Organisms to in the Studied Patients During 2018 - 2022 (N = 592)
| Organism Drug | Acinetobacter | Staphylococcus | Stenotrophomonas | Escherichia coli | Enterococcus | Pseudomonas | Klebsiella | Acinetobacter |
|---|---|---|---|---|---|---|---|---|
| Oxacillin | ||||||||
| Resistant | - | 46 (38.0) | - | - | - | - | - | - |
| Sensitive | - | 75 (62.0) | - | - | - | - | - | - |
| Ampicillin | ||||||||
| Resistant | - | - | - | 10 (100.0) | 14 (58.3) | - | - | - |
| Sensitive | - | - | - | 0 (0.0) | 10 (41.7) | - | - | - |
| Amikacin | ||||||||
| Resistant | 37 (72.5) | - | 18 (94.7) | 5 (8.5) | - | 15 (27.3) | 15 (28.3) | 2 (9.1) |
| Sensitive | 14 (27.5) | - | 1 (5.3) | 54 (91.5) | - | 40 (72.7) | 38 (71.5) | 22 (90.9) |
| Penicillin | ||||||||
| Resistant | - | 189 (88.3) | - | - | 5 (50.0) | - | - | - |
| Sensitive | - | 25 (11.7) | - | - | 5 (50.0) | - | - | - |
| Gentamicin | ||||||||
| Resistant | 3 (60.0) | 30 (16.49) | - | 0 (0.0) | - | - | 1 (16.7) | - |
| Sensitive | 2 (40.0) | 153 (83.6) | - | 7 (100.0) | - | - | 5 (83.3) | - |
| Cefepime | ||||||||
| Sensitive | 22 (78.6) | - | 9 (90.0) | 23 (56.1) | - | 14 (29.8) | 16 (55.2) | 3 (20.0) |
| Resistant | 6 (21.4) | - | 1 (10.0) | 18 (43.9) | - | 33 (70.2) | 13 (44.8) | 12 (80.0) |
| Ceftazidime | ||||||||
| Resistant | 41 (89.1) | - | 20 (95.2) | 42 (76.4) | - | 26 (59.1) | 29 (64.4) | 5 (23.8) |
| Sensitive | 5 (10.9) | - | 1 (4.8) | 13 (23.6) | - | 18 (40.9) | 16 (35.6) | 16 (76.2) |
| Cefotaxime | ||||||||
| Resistant | 43 (79.6) | - | 19 (100.0) | 51 (85.0) | - | 6 (75.0) | 36 (69.2) | 6 (28.6) |
| Sensitive | 11 (20.4) | - | 0 (0.0) | 9 (15.0) | - | 2 (25.0) | 52 (30.8) | 15 (71.4) |
| Cefixime | ||||||||
| Resistant | - | 56 (51.4) | - | - | - | - | - | - |
| Sensitive | - | 53 (48.6) | - | - | - | - | - | - |
| Ciprofloxacin | ||||||||
| Resistant | 25 (59.5) | 94 (51.6) | 1 (9.1) | 36 (70.6) | 16 (84.2) | 7 (16.7) | 32 (66.7) | 3 (13.0) |
| Sensitive | 17 (40.5) | 88 (48.4) | 10 (90.9) | 15 (29.4) | 3 (15.8) | 35 (83.3) | 16 (33.3) | 20 (87.0) |
| Chloramphenicol | ||||||||
| Resistant | - | 32 (27.8) | 0 (0.0) | 0 (0.0) | - | - | 0 (0.0) | - |
| Sensitive | - | 83 (72.2) | 6 (100.0) | 5 (100.0) | - | - | 6 (100.0) | - |
| Clindamycin | ||||||||
| Resistant | - | 128 (56.9) | - | - | - | - | - | - |
| Sensitive | - | 97 (43.1) | - | - | - | - | - | - |
| Co-trimoxazole | ||||||||
| Resistant | 10 (55.6) | 28 (28.6) | 2 (8.3) | 12 (75.0) | - | - | 8 (50.0) | 2 (28.6) |
| Sensitive | 8 (44.4) | 70 (71.4) | 22 (91.7) | 4 (25.0) | - | - | 8 (50.0) | 5 (71.4) |
| Levofloxacin | ||||||||
| Resistant | 7 (63.6) | 2 (33.3) | 0 (0.0) | 9 (75.0) | - | - | 4 (40.0) | - |
| Sensitive | 4 (36.4) | 4 (66.7) | 25 (100.0) | 3 (25.0) | - | - | 6 (60.0) | - |
| Meropenem | ||||||||
| Resistant | 41 (85.4) | - | 13 (86.7) | 9 (16.7) | - | 28 (59.6) | 21 (44.7) | 3 (18.8) |
| Sensitive | 7 (14.6) | - | 2 (13.3) | 45 (83.3) | - | 19 (40.4) | 26 (55.3) | 16 (81.3) |
| Vancomycin | ||||||||
| Resistant | - | 4 (36.4) | - | - | 22 (91.7) | - | - | - |
| Sensitive | - | 7 (63.6) | - | - | 2 (8.3) | - | - | - |
In the univariate logistic regression analysis, all variables except gender and age showed statistically significant associations with catheter-related mortality. For each day increase in the interval between patient admission and infection onset, the odds of death increased by 5% (P < 0.001). Furthermore, the univariate analysis indicated that gram-negative bacteria increased the odds of death by 75% in patients with catheter infections (P = 0.01) (Table 3).
Table 3.Logistic Regression Analysis for Survival Status of the Patients with Catheter Infections During 2018 - 2022 (N = 592)
| Variables | Crude OR (95% CI) | P-Value | Adjusted OR (95% CI) | P-Value |
|---|---|---|---|---|
| Sex | ||||
| Female | 1 | - | - | - |
| Male | 1.01 (0.67, 1.54) | 0.943 | - | - |
| Age | 1.01 (1.0, 1.03) | 0.054 | - | - |
| Sample culture | ||||
| Shaldon | 1 | - | 1 | - |
| Blood | 3.65 (2.36, 5.65) | < 0.001 | 2.82 (1.78, 4.49) | < 0.001 |
| Catheters place | ||||
| Jugular vein | 1 | - | 1 | - |
| Femoral | 0.5 (0.32, 0.79) | 0.003 | 2.83 (1.09, 7.32) | 0.032 |
| Others | 0.41 (0.18, 0.96) | 0.039 | 1.22 (0.46, 3.22) | 0.684 |
| The time interval between hospitalization and infection | 1.05 (1.03, 1.07) | < 0.001 | 1.05 (1.03, 1.07) | 0.001 |
| Hospitalization period | 1.03 (1.02, 1.05) | < 0.001 | - | - |
| Time interval from implantation to infection | 0.98 (0.97, 0.99) | 0.001 | 0.98 (0.96, 0.99) | 0.001 |
| Organism | ||||
| Gram-positive | 1 | - | - | - |
| Gram-negative | 1.75 (1.14, 2.67) | 0.01 | - | - |
In the multivariate logistic regression analysis, several factors demonstrated significant associations with the odds of death in patients, including catheter placement in the femoral vein compared to the jugular vein (P = 0.032), blood culture samples compared to Sheldon samples (P < 0.001), duration from admission to infection (P < 0.001), and duration from catheter insertion to infection (P < 0.001). According to our results, the odds of death from catheter infection when placed in the femoral vein were 2.83 times higher than when placed in the jugular vein (OR = 2.83, 95% CI = 1.09 to 7.32).
5. Discussion
The present study aimed to investigate the epidemiology of CRBIs, associated factors, mortality rate, and factors associated with death in patients with this infection. Our results showed that the most common microorganisms associated with catheter-related infections in HD patients were Staphylococcus, E. coli, and Pseudomonas, respectively. Additionally, these microorganisms exhibited the highest drug resistance. The mortality rate in patients with CRBI was approximately 20%. Gram-negative bacteria increased the risk of death from catheter infection by 75% compared to gram-positive bacteria. Placement of the catheter in the femoral vein compared to the jugular vein, and blood culture samples compared to Sheldon samples, increased the risk of death by approximately 2.83 times. The duration of hospitalization until infection onset showed up to a 5% increase in the mortality rate.
In line with our findings, Opoku-Asare et al. also reported a higher prevalence of gram-negative bacteria than gram-positive bacteria. Among the gram-positive bacteria, Acinetobacter baumannii and coagulase-negative Staphylococcus had the highest prevalence in patients (4). Our findings regarding the predominance of gram-positive Staphylococcus bacteria in CRBI are consistent with Opoku-Asare et al (4). However, broader epidemiological evidence suggests a stronger link between gram-negative bacteria and catheter infections, which was not the primary focus of our study. Epidemiological studies have generally reported a stronger association between gram-negative bacteria and catheter infections than gram-positive bacteria, as research has shown that in contaminated environments, the growth of gram-negative bacteria, including bacilli, increases (20, 21). Other catheter infections caused by gram-negative bacteria include Pseudomonas aeruginosa, E. coli and Klebsiella (22, 23).
The findings from a retrospective study in China (2021) that examined the risk of central venous diseases causing microbial colonization in HD patients are consistent with our study. The most common type of microorganism associated with gram-positive infections was the epidermidis species, similar to our findings. Liang et al. found that CRBI in the central vein was more common than in other sites, and the most prevalent microorganisms were coagulase-negative Staphylococcus species and S. aureus, aligning with our results (24). The findings of a cohort study by Mohamed et al. were also consistent with our study regarding catheter placement sites and microbial species. This similarity may be attributed to the study population and age group examined, as both studies reported a mean patient age of 60 years or older (25). The increased risk of infection, particularly CRBI, with prolonged central venous catheter use in end-stage renal disease patients can be attributed to impaired immunity, comorbidities, malnutrition, and frequent catheter use during HD (26).
The retrospective study by Zanoni et al. in Italy, a three-year longitudinal investigation of HD patients, also reported similar findings to our study, with the highest rates of CRBI caused by gram-positive bacteria, particularly S. aureus, and a higher incidence of infections with catheters placed in the jugular vein compared to the femoral vein (27). The catheter insertion site can significantly influence the incidence of infection. The anatomical location of the femoral vein presents a conducive environment for bacterial growth due to its high moisture content and slower blood flow.
While the specific microorganisms responsible for CRBI can vary across studies, the predominance of gram-negative bacteria is often attributed to the high rates of urinary, gastrointestinal, and diabetic foot infections in HD patients. Additionally, the duration of hospital stay and poor environmental hygiene can also influence infection rates (11, 28).
This study found the highest rate of catheter infections in the age group of 60 years and above. However, the study by Murea et al. on 464 HD patients in the US reported lower infection rates in those over 75 years of age. The level of satisfaction with catheters in elderly dialysis patients has been reported as contradictory. This could be related to factors such as nasal colonization, lower sweating, and reduced catheter-related activities in the elderly (29, 30).
The cross-sectional study by Wang et al. in China also reported a mean age of over 60 years in HD patients, and the most common catheter placement site was the femoral vein, consistent with our findings. The femoral vein is more prone to infections due to higher contamination and difficulty in maintaining cleanliness and hygiene (31). The rate of CRBSI depends on the quality of healthcare systems and hospital hygiene conditions. The CRBSI is a nosocomial infection, and its incidence can vary based on changes in the population at risk, the prevalent bacteria in the environment, the level of hospital contamination, and increased antibiotic use (32, 33).
In our study, the number of cases of GEN-resistant Staphylococcus was lower than for other antibiotics. This relationship could be due to the changing trend towards gram-negative species in CRBI. Wolley et al. also found that drug resistance to GEN was higher in HD patients with CRBI than in the general population. However, they failed to observe any association between the level of drug resistance and S. aureus bacteria (34, 35). Previous studies have reported that the most common microorganisms causing catheter infections are gram-positive species, including S. aureus, Staphylococcus epidermidis, Streptococcus, Enterococcus, Corynebacterium, and Candida fungi (36, 37). Additionally, the femoral site has been reported as the most common catheter placement location, and A. baumannii has shown the highest drug resistance. However, recent studies have indicated a shift towards gram-negative bacteria in drug resistance (38, 39). The differences observed between the current and past studies may be due to variations in the study populations and the emergence of different drug resistance patterns in hospitals. This is a global health concern, as it can lead to an increased disease burden and mortality (40).
5.1. Conclusions
This study showed that the mortality rate due to CRBI in HD patients is approximately 20%. The risk of mortality increases with the catheter’s location, the duration of hospitalization until the onset of infection, and the time interval between catheter placement and infection occurrence. Regarding antimicrobial resistance, the highest resistance was observed in Staphylococcus species against PEN and CLU antibiotics, while the lowest resistance was observed in E. coli against AMP, GEN, and CAM antibiotics. Given the increasing use of central venous catheters in HD patients, the risk of CRBI is likely to increase in the future. Therefore, we recommend conducting high-quality prospective studies with larger sample sizes to better evaluate this association and control the associated complications.
5.2. Strengths of the Study
Given the importance of investigating the risk factors for CRBIs in HD patients to prevent complications, this epidemiological study successfully identified the risk factors and causes associated with CRBI-related mortality in these patients. Additionally, the antibiotic resistance and susceptibility patterns of the microorganisms associated with infections were evaluated and reported, which could be effective in controlling microbial resistance in hospitals.
5.3. Limitations of the Study
The study was cross-sectional and descriptive-analytical in nature, which did not allow for the investigation of causal effects of the variables examined on the rate of CRBI in patients. Furthermore, the overlap of a portion of the study period with the COVID-19 pandemic affected patient visits and reduced the number of HD patients.