1. Background
Dental caries is defined as the local progressive destruction of tooth structure, characterized by demineralization of superficial enamel layers in acids caused by the fermentation of carbohydrates (1, 2). Orthodontic appliances increase the retention of dental plaque on the tooth surface. Following the placement of orthodontic appliances in the oral cavity, the oral microbial flora quickly shifts to acidogenic bacteria, resulting in the formation of white spot lesions (WSLs) around orthodontic brackets in about one-third of patients (3, 4). Moreover, dental caries are difficult to detect during orthodontic treatment because the teeth are covered with orthodontic brackets (5).
Education and training of orthodontic patients to adhere to oral hygiene measures and permanent behavioral change of patients for caries prevention are effective but hard to achieve (6). Fixed appliances impede access to tooth surfaces and increase the complexity of mechanical cleaning for patients. This highlights the importance of adjunctive measures to minimize the incidence of dental caries (7).
Fluoridated compounds are among the most effective caries prevention products, which are used for the prevention of WSLs. They are available in the form of mouthwash, gel, varnish, etc. (3). One advantage of fluoride varnish is that it is effective even in the presence of dental plaque and does not require tooth cleaning before its application (8). However, limited effects of fluoride on pit and fissure caries and the risk of overexposure of patients to fluoride, as well as the general recommendations on limiting fluoride consumption, have decreased the popularity of fluoride compounds (9). Antibacterial agents, such as chlorhexidine, lack supporting evidence concerning their efficacy. Moreover, they often cause the discoloration of bracket bonding agents and adversely affect dental esthetics (10). Laser irradiation is another suggested modality that changes the structure of enamel crystals and can prevent enamel caries in fixed orthodontic patients. However, this modality requires further investigations and has some contradictions (6, 11).
The dependence of fluoride compounds on the salivary calcium and phosphate ions has focused the attention of researchers towards the production of calcium- and phosphate-based remineralizing agents (9). Tooth mousse, first produced by Reynolds et al. cited in Chambers et al., is among these products that contain casein phosphopeptide amorphous calcium phosphate (CPP-ACP) (10). As known, CPP prevents the adhesion of oral bacteria to saliva-coated hydroxyapatite. It selectively inhibits the adhesion of streptococci to tooth surfaces and can change the dental plaque microbial flora, resulting in less accumulation of cariogenic bacterial species such as oral Actinomyces (9).
Besides, MI Paste Plus is a recently introduced product suggested for treating incipient caries, which is composed of CPP-ACP and 900 ppm fluoride. Simultaneous application of CPP-ACP and fluoride can exert a synergistic effect. This product has shown promising results for caries control (9, 12, 13).
As mentioned earlier, dental caries is a public health dilemma, affecting a considerable number of fixed orthodontic patients. Several methods have been suggested to prevent and control caries in orthodontic patients; however, each method has its advantages and shortcomings. More recent studies have focused on CPP-ACP use, but controversial results have been reported regarding its caries prevention efficacy (14-16). A large number of studies on this topic have been conducted in vitro. Clinical studies have mainly focused on its application after orthodontic treatment completion (3, 17-21), while the incidence of caries drops significantly after bracket deboning (5).
Considering the high risk of caries during orthodontic treatment, the application of remineralizing agents seems to be a conservative approach.
2. Objectives
This study aimed to compare the efficacy of MI Paste Plus and fluoride varnish remineralizing agents to prevent WSLs in fixed orthodontic patients.
3. Methods
The inclusion criteria were healthy males and females aged 12 to 35 years, no systemic disease, no syndromic anomalies, and no allergy to milk protein or benzoate preservatives. The exclusion criteria included patients whose orthodontic treatment would be completed in less than six months, patients with physical or mental disabilities, alcoholics and substance abusers, and unwillingness to participate in the study.
After obtaining ethical approval from the university's ethics committee, necessary arrangements were made with an orthodontist to refer patients on fixed orthodontic treatment to the university. He was requested to randomly refer young adult patients visiting during four working days to the dental school for participation in the study.
3.1. First Visit
All patients were visited in four sessions within four working weeks. The patients were first briefed about the study, and written informed consent was obtained from them. Next, data including age, education level, and systemic health status were recorded in predesigned datasheets. Clinical examination was performed using a dental mirror and an explorer. The DMFT and plaque index of patients were calculated and recorded. Patients requiring dental treatments were referred to the respective departments.
3.2. Grouping of Patients
After data collection, 60 patients were randomly divided into the following four groups to standardize the groups in terms of patient adherence to oral hygiene measures according to their plaque index:
(A) Plaque index < 50%: 9 patients
(B) 50%≤ plaque index < 70%: 12 patients
(C) 70% ≤ plaque index < 80%: 24 patients
(D) 80% ≤ plaque index ≤ 100%: 15 patients
The patients in each of the aforementioned groups were then randomly divided into three subgroups. Table 1 presents the properties of the materials used in this study.
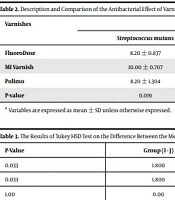
Table 1.Material Comparison
| Substance | Ingredient | Mechanism of Action |
|---|---|---|
| Fluoride varnish | Fluoride | Blockage of bacterial enzymes; Inhibition of demineralization; Progression of remineralization |
| MI Paste Plus | Casein phosphopeptides-amorphous calcium phosphate; Fluoride; Xylitol | Stabilization of calcium and phosphate on the enamel surface; Synergic effect of fluoride and CPP-ACP |
3.3. Second Visit
In the second visit, the patients’ saliva pH was measured using a pH kit (Merck, Germany). This was done by placing the pH-meter strip in the saliva and comparing the obtained color with the standard chart on the kit's label (Figure 1).

Figure 1.
The pH kit
Next, the patients’ teeth were clinically examined using a dental mirror, an explorer, and air spray under the dental unit light. The presence and severity of WSLs were evaluated and recorded using the International Caries Detection and Assessment System. The date of intervention initiation was also recorded for each patient (Table 2).
Table 2.International Caries Detection and Assessment System Index
| Code Description | |
|---|---|
| 0 | Intact |
| 1 | The first observable change in tooth enamel (it can be seen just after prolonged drying by air, or it is confined to the pit or fissure area) |
| 2 | An observable and distinct change in enamel |
| 3 | Local breakdown of enamel (without visible clinical symptoms of crown involvement) |
| 4 | The dark shadow of dentine which is localized below |
| 5 | Evident cavity with a visible dentine |
| 6 | An extensive evident cavity with visible dentine |

Figure 2.
The enrollment, random allocation, follow-up, and analysis of study participants flowchart
Next, according to the group allocation of patients, the MI Paste Plus group received verbal instructions on the correct use of this product (frequency, amount, and time of use) according to the manufacturer’s instructions. The patients were instructed to use a pea-sized amount of the paste every night after toothbrushing (once a day) (Figure 2).
In the fluoride varnish group, fluoride varnish was applied to the teeth. The patients were requested to spit out their saliva five minutes after use and refrain from eating and drinking for three hours. They were also asked to refrain from toothbrushing for 24 hours. Measurement of the saliva pH and grading of WSLs were the only procedures performed in the control group.
In this session, all patients were scheduled for a follow-up session (first follow-up) two months later. In the third (first follow-up) and fourth (second follow-up) visits scheduled two months after the first follow-up, the International Caries Detection and Assessment System Score was determined. In the fluoride varnish group, fluoride varnish was applied. In the MI Paste group, patients were questioned about the amount and method of paste use, and their questions were answered.
3.4. Fifth Visit (Third Follow-up)
About two months after the fourth visit, each patient was contacted and reminded about the subsequent follow-up. In the third follow-up, the saliva pH was measured (compared with the baseline value). All procedures performed in previous follow-ups were also repeated in this session. Also, all patients underwent a thorough clinical examination of their teeth for dental caries. They were referred to respective specialists in case of requiring restorative treatments.
The mean and standard deviation of quantitative variables were reported and analyzed using one-way ANOVA. Repeated measures ANOVA was applied to compare the groups regarding the respective indices. The Bonferroni adjustment was applied for pairwise comparisons of the groups.
4. Results
The DMFT scores at the onset of fixed orthodontic treatment are shown in Table 3. As shown, there was no significant difference in baseline data between the study groups (P = 0.442).
Table 3.Comparison of DMFT Scores in Three Groups Before Intervention
| Group | Mean ± SD | P-Value |
|---|---|---|
| Control | 3.95 ± 3.3 | 0.442 |
| Varnish | 2.75 ± 2.7 | |
| MI Paste | 3.45 ± 2.7 |
Table 4 presents the results of ANOVA regarding the effect of assessment time and intervention type on WSLs. As shown, there was a significant difference among the groups in the score of WSLs (P = 0.021), which was due to the difference between the control and MI Paste Plus groups (P < 0.05).
Table 4.Comparison of WSLs Score in Three Groups by Repeated Measures ANOVA
| Source of Variations | Sum of Squares | Degree of Freedom | Mean of Squares | F | P-Value |
|---|---|---|---|---|---|
| Time | 4.434 | 1 | 4.434 | 1.300 | 0.259 |
| Time × WSLs (before intervention) | 78.940 | 1 | 78.940 | 23.141 | < 0.001 |
| Time × group | 28.477 | 2 | 14.238 | 4.174 | 0.020 |
| WSLs (before intervention) | 687.707 | 1 | 687.707 | 107.974 | < 0.001 |
| Intervention group | 53.106 | 2 | 26.553 | 4.169 | 0.021 |
Table 5 shows the mean saliva pH in the three groups after six months and the WSLs score after two, four, and six months.
Table 5.Mean Saliva pH in Three Groups After Six Months and WSLs Score After Two, Four, and Six Months
| Index | Mean ± SD | P-Value |
|---|---|---|
| Saliva pH at six months | 0.814 | |
| Control | 6.45 ± 0.6 | |
| Varnish | 6.45 ± 0.5 | |
| MI Paste | 6.45 ± 0.5 | |
| WSLs score at two months | 0.472 | |
| Control | 2.75 ± 3.2 | |
| Varnish | 1.65 ± 1.8 | |
| MI Paste | 2.25 ± 3.1 | |
| WSLs score at four months | 0.017 | |
| Control | 3 ± 3.1 | |
| Varnish | 1.15 ± 1.3 | |
| MI Paste | 1.3 ± 1.6 | |
| WSLs score at six months | 0.034 | |
| Control | 3.15 ± 2.9 | |
| Varnish | 1.6 ± 1.6 |
Pairwise comparisons of the groups with Bonferroni adjustment revealed a significant difference between the control and MI Paste Plus groups (mean diff. = 1.23 ± 0.4, P = 0.033). The differences between the control and varnish (P = 0.078) and MI Paste Plus and varnish (P > 0.999) groups were not significant. The change in the mean WSLs score was not significant over time in the control group (P = 0.378). As shown in Figure 1, the trend of change in the WSLs score was almost horizontal in the control group while descending in other groups. However, the trend of WSLs score reduction was steeper in the MI Paste Plus group than in the varnish group.
5. Discussion
White spot lesions (WSLs) are the initial phase of caries development, characterized by demineralization of subsurface enamel without cavitation. White spot lesions can progress and create a cavitated lesion. These lesions develop in a high percentage of orthodontic patients (6, 20). Several materials are used to treat WSLs, such as fluoridated toothpaste, fluoridated mouthwashes, fluoride varnish, and CPP-ACP. Each of these products has a different mechanism of action in preventing WSLs, and each has its advantages and disadvantages. Studies conducted on the efficacy of these products have shown controversial results and mainly concentrated on the post-orthodontic phase (14-16). Thus, the present study compared the efficacy of fluoride varnish and MI Paste Plus to prevent WSLs in orthodontic patients.
The mean score of WSLs in the control group decreased by 0.2 units during six months, which was not statistically significant. In a study by Robertson et al. (22), the control group showed a 91% increase in WSLs, highlighting the significance of patients' oral hygiene instruction at the study onset. Other studies evaluated WSLs after orthodontic treatment or in-vitro; thus, their results cannot be compared with ours.
In this study, the mean score of WSLs in the MI Paste Plus group after two months of intervention showed a significant reduction by 2.9 units; this reduction was 3.85 units after four months. The WSLs score reduction was expected considering the cariostatic properties of fluoride and CPP-ACP. However, the difference between the baseline value and the value at six months was insignificant. A possible reason for the decreased efficacy of the materials may be the reduced motivation of patients during the long course of the study.
In pairwise comparisons of the groups, the difference between the control and MI Paste Plus groups was significant such that the MI Paste Plus group experienced a greater reduction (1.23) in the mean score of WSLs during six months compared with the control group. Similar results were reported by Robertson et al. (22) and Abdoli (23). However, Ballard et al. (24), Huang et al. (12), and Beerens et al. (25) found no significant difference between the intervention and control groups in this respect. Nevertheless, the duration of these studies was less than three months, which may explain the differences in the results. In the present study, MI Paste Plus was used according to the manufacturer’s instructions. However, its application method was variable in previous studies, which could have affected the results.
The superior results of MI Paste Plus compared with the control group can be due to its mechanism of action. As known, MI Paste Plus is composed of fluoride and CPP-ACP. Fluoride decreases enamel demineralization and enhances enamel remineralization. It also inhibits metabolic enzymes in cariogenic bacteria (3, 6, 26). On the other hand, CPP-ACP causes the accumulation of calcium and phosphate on the enamel surface and results in enamel remineralization. Besides, CPP prevents the attachment of oral bacteria to saliva-coated hydroxyapatite on the enamel surface. It selectively inhibits the attachment of streptococci and changes the microbial flora of dental plaque, resulting in less colonization of cariogenic species such as oral Actinomyces. Elevated levels of calcium and fluoride ions in the tooth surface and within the dental plaque inhibit acid production, while phosphate ions contribute to buffering plaque pH changes. As a result, the combined application of CPP-ACP and fluoride exerts synergistic effects (26).
Pairwise comparisons of the groups revealed that the mean WSLs score reduction within six months in the varnish group was 1.05 units higher than that in the control group, although this difference was insignificant. The mean score of WSLs decreased by 0.85 units in the varnish group at six months, but this reduction was not significant either. Huang et al. (12) and Singh et al. (16) reported similar results and showed that the varnish group had no superiority over the control group. However, Stafford (27) and Lopatiene et al. (15) reported that varnish application was effective; however, they evaluated patients after the completion of orthodontic treatment. Thus, enhanced adherence to oral hygiene measures may explain the difference in the results. A more recently published paper by Flynn et al. (28) reported that fluoride varnish had no superior advantage in reducing WSLs during orthodontic treatment. A recent systematic review conducted on the efficacy of fluoride varnish for treating orthodontically-induced WSLs pointed to this controversy and stated that adequate data are not available to draw a definite conclusion (29).
Pairwise comparisons showed that the mean WSLs score reduction in the MI Paste Plus group was higher than that in the varnish group by 0.17 units at six months in the current study; however, this difference was not significant. In the study by Huang et al. (12), the difference between the MI Paste Plus and varnish was insignificant (12). However, Llena et al. (14) demonstrated that MI Paste Plus was more effective than varnish. Nevertheless, this difference was only significant in the first four weeks of the 12-week study period. The superior efficacy of MI Paste Plus compared with fluoride varnish can be due to the presence of calcium and phosphate ions along with fluoride because fluoride requires six phosphate ions and 10 calcium ions for the formation of fluorapatite. Therefore, in the case of only using fluorinated compounds, these ions may not be available in adequate amounts (30).
Also, in fluorinated products, the precipitation of calcium fluoride on the surface of WSLs may inhibit the passage of ions into the deeper, more affected layers (30). On the other hand, when CPP-ACP is used, neutral ions such as CaHPO4 are produced, localized on the tooth surface, and subsequently diffuse deep into the body of WSLs; accordingly, remineralization occurs throughout the entire body of WSLs (31).
The mean saliva pH in the control group was 6.8 at baseline and 6.45 after the intervention. The mean pH was 6.35 before and 6.45 after the intervention in the varnish group. In the MI Paste Plus group, the mean pH was 6.45 before and 6.35 after the intervention. However, in general, no significant difference was noted in pH after the intervention compared with baseline. In a study by Heshmat et al. (32), the saliva pH in the MI Paste Plus group did not change significantly after the intervention compared with baseline. Another study reported the saliva pH increase after the intervention; this result may be due to patients' oral hygiene and diet (33). Different results regarding the saliva pH in different studies may be due to the tools used to measure pH. Also, a recent study comparing the efficacy of CPP-ACP with/without fluoride reported that exercise and innate metabolic differences might affect the pH (34). In the present study, a pH-meter (Merck, Germany) was used, which was not digital and could not measure changes smaller than one unit. The groups were not fundamentally different in terms of mean age, gender, education level, plaque index, DMFT, or WSLs score at baseline. Thus, these factors had no significant confounding effect on the results.
As mentioned earlier, most previous studies had been conducted in the short term (12, 14, 22, 24, 26) and had an in vitro design or conducted on patients after completing their orthodontic treatment. However, the current study was unique as it evaluated patients during orthodontic treatment. However, in the present study, patients had different levels of cooperation due to their decreased motivation over time. This was especially true in the last months of the study. Also, in the present study, clinical examination of oral cavity and dentition was performed with an explorer under unit light. This may explain the difference in the results compared with studies that performed clinical dental examinations using other tools. In general, scientific evidence supporting the remineralizing treatments of WSLs is not conclusive, and controlled clinical trials with long-term follow-ups are required to obtain more accurate results (35).
5.1. Conclusions
Under the limitations of this study, during orthodontic treatment, the number of WSLs in the control group slightly decreased following conventional oral hygiene. Both MI Paste Plus and fluoride varnish decreased the formation of WSLs in orthodontic patients. Besides, MI Paste showed superior results compared with fluoride varnish, but not significantly. Also, MI Paste Plus and fluoride varnish had no significant effect on the saliva pH.