


1. Background
To reduce educational inequality and bridge the gap between academic achievement and success among girls and boys of all groups, races, ethnicities, and geographical areas, developed countries attempt to make changes and improvements in their educational systems every year and spend large amounts of money on educational planning (1). Educational equality is defined as the presence of equal educational opportunities for most members of society to prepare themselves for active and comprehensive participation in the community regardless of financial, social, and cultural pressures (2).
Justice in the educational environment is attained when learners are able to achieve scientific, educational, religious, moral, and social goals through the available inputs and processes in the educational environment. In the first dimension of educational justice, equality signifies that economic, social, ethnic, or physical status should not affect the educational process. Educational justice does not pertain to allocating resources and equal attention to all people, but rather, it implies allocating resources and paying attention to the conditions of all learners. Since the conditions of learners in training courses largely differ, educational justice is considered to be the most fundamental dimension of organizational justice, affecting all areas of education and providing the opportunity for the emergence of talents and capabilities at the macro-level (3).
The educational activities of every country may be considered an investment of one generation for another. In fact, the material and non-material costs incurred in training are considered to be investments in human resources as education provides an opportunity for the productivity of the individual and society under the right circumstances.
Equitable distribution of educational facilities in institutions is a controversial issue in the field of humanities (4). Any country aiming to have comprehensive, balanced, and sustainable development should first develop its higher education systems, research, and technology in a balanced and sustainable manner. Providing opportunities to reduce educational inequality is a pillar of achieving balanced and sustainable development in higher education. Such a mitigation in inequality results in the provision of equal and fair educational opportunities to all students. On the other hand, higher education in the field of medical sciences (higher health education) is of particular importance given the priority of health issues as an axis of sustainable development. Medical sciences are part of the resource production performance in the national health system, which undeniably impacts the functions of the health system. Such examples of these impacts are the provision of manpower, knowledge production, influence on the provision of services, and the improvement of health and sociocultural/economic development.
Identifying the current state of inequality in this area is the first step toward creating an equal opportunity for education. Measuring the level of inequality in higher education is important as inequality reduces productivity. Development of educational equality in medical sciences is essential to improving justice in health, education, and technological development, which will eventually result in economic growth (5). In addition, numerous universities in different countries pay attention to improving the health of the international community in their organizational mission. Therefore, research in this regard is a major task to meet the needs of the health sector on different levels.
McDonough & Fann (2007) considered individual, institutional, and contextual factors to be the influential factors in entering higher education. In this context, the individual level indicates the barriers to access higher education due to individuals' circumstances and characteristics, such as economic and social status or educational background. The institutional level of schools and colleges plays a key role in the formulation, selection, and prioritization of university admissions. The contextual level refers to a complex network of factors that involve individuals, organizations, and inter-organizational interactions (6). According to Uribe Correa (2012), various dimensions of access to higher education include access as the capacity to absorb demand (access as the presence of sufficient seats in a system from a supply perspective) and access as social justice (equality known as a social value in academic societies implying equal opportunities for every individual) (7).
Among various universities and disciplines across the world, medical universities have been the place of major conflicts over basic political, economic, social, and cultural issues due to their strategic position (8). According to Rajabi et al., justice in higher education is directly correlated with justice in health since public health promotion is the primary gal of medical education. Some of the most important reforms in medical education are the integration of medical education with the service delivery system in 1985 and the formation of the Ministry of Health, Treatment, and Medical Education (9). Such changes facilitate the growth and development of health and medical sciences through the establishment and development of universities and medical schools in various provinces of the country. In numerous Asian countries (including Iran), medical universities have not been able to achieve this goal despite the advancement of medical sciences (10).
Research on educational inequality plays a pivotal role in monitoring and evaluating educational development processes and is a potent tool for assessing the progress of educational development in a country. Chabok et al. (11) conducted a study using the scattering coefficient model to measure the degree of inequality in the schools of Urmia University of Medical Sciences (Iran) based on various indicators. The obtained results indicated that among the schools of Urmia University of Medical Sciences, the highest inequality rate was 0.8 in the input indices, and the lowest inequality rate was 0.41 in the output indices. According to Yazdi Feyzabadi et al. (5), inequalities are significant in indices such as the number of the fields of study in some graduate courses, the number of students by gender, and the education budget despite the reduction of inequalities in other educational indicators. To provide equal educational opportunities, politicians have also paid attention to the balanced development of educational infrastructures in different provinces in Iran.
In another study, Eafati et al. (12) reported a significant and direct correlation between the indicators of the independent variables of the family context, school process, output and outcomes, and input with the dependent variable of educational inequalities. Using the scattering coefficient model, Sameri et al. (13) also reported the highest level of inequality to be 0.828 in student indicators and the lowest level of inequality to be 0.3 in academic achievement indicators. Furthermore, Wink Junior & Zanandrea Paese (14) stated that regions with the highest inequality in education were poorest in terms of socioeconomic status in Brazil.
Parental education and socioeconomic status are considered to be the opportunities and conditions with the greatest power to explain inequalities. In this regard, Ataç (15) claimed that each of these parameters could be specific and practical approach to understanding the impact of students' socioeconomic backgrounds on their academic achievement. Another issue is causal correlations based on socioeconomic variables and geographical changes, which lead to partial regional inequalities in Turkey. The findings of Gorard et al. (16) showed that differences in living conditions, gender, ethnicity, native language, family structure and size, parental income and education, social class, and housing status are among the significant influential factors in inequality in access to higher education.
2. Objectives
The present study aimed to evaluate the determinants of equal access to higher health education opportunities to help managers and planners develop a model for reducing inequality at Kermanshah University of Medical Sciences (KUMS) and adopt appropriate strategies to address inequalities in this regard.
3. Methods
In this cross-sectional applied study, data were collected from documents field information, and the research tool was a questionnaire. The study population included the students of KUMS in the academic year 2020 - 2021. The participants were selected from seven schools of health, nursing and midwifery, paramedicine, dentistry, pharmacy, medicine, and nutrition (n = 5,390). In total, 358 students were selected via stratified sampling using the Cochran formula. The number of the samples was determined in proportion to the population of the students per each school after extracting the total sample size in KUMS. The final samples were randomly selected from each school. The sample size selected from the schools of KUMS are shown (Table 1).
| School | Statistical Population | No. of Male Samples | No. of Female Samples | Total |
|---|---|---|---|---|
| Medicine | 1,962 | 61 | 69 | 130 |
| Health | 415 | 7 | 21 | 28 |
| Nursing and midwifery | 774 | 22 | 30 | 52 |
| Pharmacy | 504 | 15 | 18 | 33 |
| Dentistry | 421 | 16 | 12 | 28 |
| Paramedicine | 941 | 29 | 33 | 62 |
| Nutrition | 370 | 7 | 18 | 25 |
| Total | 5,390 | 157 | 201 | 358 |
Some of the data was collected through a field survey using a questionnaire, and the other data were acquired by reviewing the documents. The field data collection tool consisted of two main sections; the first section was about contextual indicators such as demographic questions regarding the individual, social, and economic characteristics of the students' families. The second section contained questions about educational indicators such as input, process, and output. Notably, data on the inputs of the educational system were collected using documents through synchronous systems and Azarakhsh personnel system and research information management. The required statistics provided by the deputies and departments of the KUMS schools.
Process indicators were obtained by the Montez Yorke higher education process quality questionnaire (17) and Huang's social and scientific interaction as quoted by Omidifar (18). Output indicators were obtained using other questionnaires, such as Schneider’s questionnaire as quoted by Najjari & Hassani (19), Keys' social welfare as quoted by Goodarzi et al. (20), Prado’s cultural intelligence (21), social problem-solving by D’Zurilla et al., standardized by Mokhberi et al. (22), job search skills by Waryszak & King (23), attention to health by Sijtsema et al. (24), and attention to the environment by Fraj & Martinez (25).
The educational indicators selected to assess the educational inequalities in KUMS were input components such as physical resources, human resources, research, education, and students, process components such as service quality, social interaction, practical interaction, teaching quality, and educational evaluation, and output components such as graduates, GPA, life expectancy, social participation, social trust, cultural intelligence, problem-solving skills, job search skills, health attention, and environmental attitude.
Opinions of educational science experts in KUMS were used to evaluate the coefficient of representation and increase reliability to determine the face validity of the questionnaire. The required corrections were made to the questionnaire based on the provided opinions and suggestions. The construct validity of the research tool was also examined as a factor, and factor analysis was performed using principal component analysis with VARIMAX rotation and exploratory analysis. The KMO coefficient was estimated at 0.801 (P < 0.001; Bartlett’s test = 9,797.120), which indicated the appropriate quality of the samples and the selected variables for the factor analysis.
In this study, 30 questionnaires were initially distributed among the students to evaluate the reliability of the instrument. Following that, a reliability test was performed on the questionnaire using the formula of Cronbach's alpha coefficient. The reliability coefficient of the entire questionnaire was calculated at 0.849, and all the coefficients are above 0.7, which confirmed their reliability and indicated the internal consistency of the variables based on the measurement of the concepts. Therefore, the validity and reliability of the research instrument were confirmed.
The educational indicators of the TOPSIS multi-criteria decision model were used to rank the schools of KUMS in terms of the status of endowments, and the Shannon entropy method and cluster analysis model were also applied for weighting. Data analysis was performed in SPSS and the Excel software.
4. Results
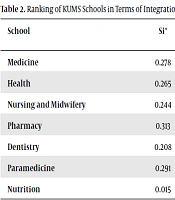
The TOPSIS model was used to investigate the status of the KUMS schools in terms of having the studied educational indicators, including contextual, input, process, and output indicators (integrated index). The obtained results showed that the schools of pharmacy and paramedical sciences were less privileged in this regard, while the schools of medicine, health, nursing and midwifery, and dentistry were semi-privileged, and the school of nutrition was privileged (Table 2).
| School | Si* | Si | Si* + Si- | Final Coefficient of TOPSIS | Cluster Analysis Model |
|---|---|---|---|---|---|
| Medicine | 0.278 | 0.14 | 0.418 | 0.3345 | Semi-privileged |
| Health | 0.265 | 0.077 | 0.342 | 0.225 | Semi-privileged |
| Nursing and midwifery | 0.244 | 0.092 | 0.336 | 0.2747 | Semi-privileged |
| Pharmacy | 0.313 | 0.01 | 0.323 | 0.0296 | Less privileged |
| Dentistry | 0.208 | 0.141 | 0.349 | 0.4034 | Semi-privileged |
| Paramedicine | 0.291 | 0.047 | 0.339 | 0.1397 | Less privileged |
| Nutrition | 0.015 | 0.311 | 0.326 | 0.954 | Privileged |
a Source: research findings (2021).
A stepwise multiple linear regression model was employed to investigate the simultaneous effects of the independent variables on the inequality of access to higher education opportunities in the KUMS schools. The index of the integrated section, which was obtained from the TOPSIS model, indicated the inequality of opportunities in access to higher education in the KUMS schools. It was considered a dependent variable to determine the effects of the contextual indicators, process indicators, and input and output indicators on the students of the medical schools of KUMS (Table 3).
a Source: research findings (2021).
b Significance level: 0.01.
c Significance level: 0.05.
According to the information in Table 3, the regression model showed the significant effects of the independent variables on the variable of inequality of educational opportunities in the KUMS medical students (F = 590.11, P < 0.001). Furthermore, the variables of the model explained 99.7% of the variance of the dependent variable (Table 4).
| Source of Changes | Sum of Squares | Degree of Freedom | Mean Squares | F | Significance |
|---|---|---|---|---|---|
| Regression effect | 0.704 | 2 | 0.352 | 590.11 | < 0.001 |
| Remaining | 0.002 | 4 | 0.001 | ||
| Total | 0.706 | 6 | - |
a Source: research findings (2021).
The variance inflation factor (VIF) test was used to determine the correlation between the independent variables. If the value of the VIF statistic is 1-5, there is no correlational problem. In the present study, the VIF statistic showed no correlations between the independent variables. Based on the extracted beta, 0.579 unit could be observed, and 0.437 unit changed the variance of the equality of opportunities for access to higher health education in the KUMS schools by changing one unit in the contextual and input variables (Table 5).
| Independent Variable | B | Beta | t | Sig. | VIF | Tolerance |
|---|---|---|---|---|---|---|
| Width of origin (constant) | -0.283 | - | -14.87 | < 0.001 | - | - |
| X1 contextual indicators | 0.776 | 0.579 | 7.52 | 0.002 | 1.3 | 1.03 |
| X2 input indicators | 0.75 | 0.437 | 5.67 | 0.005 | 1.07 | 1.01 |
| Corrected explanatory coefficient = 0 | R = 0.998 | R2 = 0.997 | ||||
a Source: research findings (2021).
5. Discussion
In the present study, significant correlations were observed between the studied indicators (process, input, output, and contextual variables) and the inequality of opportunities (consolidated index) at KUMS. Furthermore, the contextual and input variables were analyzed by the multivariate regression model. Based on the extracted beta, 0.579 and 0.437 units of change were observed in the variance of the equality of opportunities for access to higher health education in the KUMS schools, along with a change of one unit in the contextual and input variables. In other words, the contextual and input variables had the most significant impact on equal access to higher health education at KUMS.
According to the studies by Eafati et al., Sameri et al., Wink Junior & Zanandrea Paese, and Ataç (12-15), the socioeconomic status of students’ families directly affect their access to educational opportunities, as well as the parental follow-up on children’s education, and the importance of the educational status of children to their parents. Moreover, Gorard et al. (16) introduced the main influential factors in inequality in access to higher education as differences in living conditions, gender, ethnicity, native language, family size and structure, parental income and education, social class, type of school, housing status, health status, quality of life, and religious background. According to the study conducted by Bloom et al. (26) in Africa, one of the challenges associated with equal access to higher education is inequality in the distribution of university budgets. This finding is consistent with the results of the present study.
Since higher education is an important and challenging public sector of every country in the 21st century, special attention must be paid to decision-makings and policies regarding the investments of this sector due to their significant impact on the development of health education. By examining various sources about the equality of educational opportunities, access of all community members to education or higher education is observed to be a major influential factor in educational justice or creating equal educational opportunities. Therefore, the results of the present study could help policymakers and education planners of medical sciences pay attention to the indicators of equality and justice in balanced educational development, as well as indicators such as expansion, growth, and development. It seems that due to reduced equality in some indicators of educational infrastructures, proper measures should be taken to develop a balanced higher education system in order to achieve higher health education in the field of medical sciences.
In general, families with low levels of individual-family indicators (especially the socioeconomic status of parents) need specific educational courses and even academic disciplines as financial contributions for their households. This could directly impact the bridging of the gaps in education inequalities both in preparation for university and during academic studies. Notably, the context index (socioeconomic status of the individual and their family) will not have a 100% effect on creating equal educational opportunities. However, individuals will have access to higher health education opportunities and may achieve sustainable educational justice through the influence of other factors such as input indicators and even process indicators, which have a direct or indirect impact on equality or inequality.
5.1. Limitations of the Study
Due to the limitations imposed by the COVID-19 pandemic and the shifting of the staff of the administrative departments of the KUMS schools, access to the information and documents was difficult. In addition, the questionnaire was one of the limitations of our study as time was wasted in the data collection process. On the other hand, lack of cooperation of some Telegram groups of the students in informing and placing the questionnaire link in the channel to conduct the research was another limitations of the study.
5.2. Conclusions
According to the results, the schools of KUMS were classified as less privileged, semi-privileged, and privileged in terms of the context, input, process, and output indicators, as well as the role of educational justice in providing equal educational opportunities to the students. Justice could be improved at the levels of health, education, and technological development by promoting educational equality in medical sciences. The following suggestions should be considered as a basis for reducing inequality and instilling justice in higher health education.
Budget inequalities of KUMS schools should be minimized, and the input and process indicators of the development programs of the university should be reconsidered by changing the views of the officials regarding the current differences and the necessary standards of these indicators. It is also suggested that based on the actual conditions and needs of students (especially in the clinical education sector), re-planning should be considered to develop fair perspectives and expand educational spaces. It is recommended that the less privileged schools of KUMS be prioritized in terms of facilities and equipment so that they could move toward achieving sustainable educational development. Furthermore, it is proposed that similar studies be conducted in other medical universities using a comparative approach to be able to generalize the findings as far as possible.
