




1. Background
Spirituality is a foundational component of health (1). The World Health Organization (WHO) is exploring the fourth dimension of health—spiritual health—and its impact on individuals' overall well-being and happiness (2). Additionally, the WHO has incorporated a spiritual dimension into the classification of diseases in the ICD-10, recognizing that spiritual health, like physical, mental, and social health, is interconnected and influences overall health. Therefore, attention to spiritual dimensions is crucial for health promotion (3).
In medical terms, spiritual health, approached from a materialistic standpoint, is a process that can aid in the treatment of physical ailments. However, from a non-medical or meaningful medicine perspective, spiritual health is a process that not only contributes to the physical treatment of patients but also holds value in mental and psychological therapy (4).
There isn't a singular definition for spiritual health, and delineating its various dimensions can be challenging. Spiritual health encompasses more than the effects of prayer and mental states on disease recovery, and it shouldn't replace conventional medical treatments or complementary medicine (5).
Furthermore, spiritual health is adjacent to physical health, ensuring spiritual well-being and encompassing capacities to comprehend the significant aspects of life experiences (6).
Spiritual health is a dynamic aspect of life, tested through life's challenges, the consistency of one's beliefs and worldview, and the quality of relationships (7). Surveys indicate that most patients regard their spiritual health as equally important as their physical health. Numerous studies have demonstrated that religious involvement and spirituality are correlated with improved health outcomes and increased life expectancy. Addressing spiritual needs during the recovery process following illness is also shown to enhance outcomes (8).
Various theories have been proposed regarding how spirituality contributes to health. It aids in decision-making, coping with stressors, and finding meaning in life's existential questions (9). Spirituality is a vital aspect of human existence, serving as a potent force connected to health, well-being, recovery, and the quest for meaning and purpose in life (10). Spiritual experiences play a significant role in understanding happiness, depression, and psychological characteristics (11).
Recognizing the spiritual dimension as a fundamental component of human health has sparked increased interest in spiritual education (12). Prayer has been found to reduce anxiety and enhance spirituality, serving as an effective coping mechanism during illness (13).
Spiritual beliefs can profoundly impact health outcomes and the doctor-patient relationship. Medical students should be prepared to address spiritual issues in patient care, and this content should be integrated into medical curricula (14). However, there is often a gap between medical students' attitudes and expectations regarding spirituality, health, and religiosity in professional education and their application in clinical practice. Some studies have shown that medical students acknowledge the importance of spirituality and religiosity in patient care but may lack adequate preparation due to time constraints. Therefore, it is imperative for medical schools to include this topic in their curricula (15).
Today, there is a growing trend towards spirituality within educational fields more so than in other domains. Education and training offer optimal settings for nurturing spirituality in individuals, emphasizing the need for educational planning that prioritizes spiritual health (16). A spiritual education program goes beyond traditional reasoning and analytical methods typically employed in education (17); it serves as a pathway to deeper understanding and personal growth (18).
In contrast, medical school curricula often lack provisions for addressing spiritual aspects, despite patients' expectations for healthcare providers to understand and acknowledge spiritual dimensions in promoting health and well-being.
In the context of transforming medical education, principles emphasizing God-centeredness, sincerity in actions, human dignity, and attention to the material and spiritual realms have been outlined. This signals a call for educators and policymakers to take proactive steps towards enhancing spiritual health education (16).
Curriculum content concerning spirituality and spiritual health ought to be integrated into educational programs. Establishing a platform for developing curriculum content is essential. It is advisable to involve a diverse group of experts to determine the appropriate content and teaching methodologies for nursing and medical education programs focused on spiritual health (19).
Given that medical students play a pivotal role in addressing various aspects of societal health, it is crucial to incorporate effective formulation and planning strategies. This involves integrating content and spiritual themes into the curriculum, fostering a conducive educational environment, providing spiritual role models, and employing effective educational strategies to enhance students' spiritual well-being during their education (20). Research indicates that while a minority of students exhibit high levels of spiritual health, the majority fall within the average range (21). Additionally, female students tend to demonstrate higher levels of spiritual health compared to their male counterparts (22). Furthermore, there exists a correlation between students' gender, employment status, degree level, and field of study with their spiritual health levels (21).
Spiritual health is significantly associated with lower levels of perceived stress and depression among nursing students (23). Moreover, enhancing spiritual health has been linked to improved academic success among students (24). Spiritual well-being fosters academic progress by fostering motivation, indicating that interventions aimed at enhancing academic performance can positively impact students' spiritual health (25).
2. Objectives
Recognizing the importance of spiritual health, our study focuses on assessing the spiritual health levels of medical students in Kermanshah, aiming to provide insights for their education and development.
3. Methods
Our research employed a cross-sectional descriptive design, focusing on medical students enrolled in the Medical Faculty of Kermanshah from the first to the fifth year. The sample size, determined using Cochran's formula, consisted of 258 individuals selected through random sampling.
Data collection utilized the standardized questionnaire for assessing spiritual health in Iranian society, developed by the Academy of Medical Sciences. This questionnaire comprises 48 questions, with 20 assessing behavior, 16 assessing tendency, and 12 assessing insight. Responses for the insight and tendency dimensions were measured on a 5-point Likert scale ranging from "completely agree" to "completely disagree," while the behavior dimension used a 5-point Likert scale ranging from "always" to "never," with the highest score assigned to "always." The reliability and validity of the questionnaire were confirmed by Amiri et al., with a Cronbach's alpha value exceeding 0.70 (26).
Based on statistical consultation, spiritual health scores were categorized as follows: Scores below 211 indicated low spiritual health, scores between 211 and 228 indicated moderate spiritual health, and scores above 228 indicated high spiritual health.
Data analysis was conducted using SPSS-23 software. Descriptive statistics, including frequencies, percentages, means, and standard deviations, were utilized to describe the demographic characteristics of the students. The t-test was employed to compare spiritual health scores across different dimensions within subgroups of qualitative variables. A significance level of P < 0.05 was adopted. Participation in the questionnaire was voluntary, and students who chose not to participate or had incomplete questionnaires were excluded from the study.
4. Results
The study comprised 258 students, with ages ranging from 18 to 34 years and an average age of 21.59 ± 2.06. Among them, 128 individuals (49.6%) were male, and 130 individuals (50.4%) were female. Regarding academic disciplines, 153 students (59.3%) were enrolled in basic sciences, while 105 students (40.7%) were in clinical sciences. In terms of living arrangements, 19.4% resided in dormitories, 73.4% lived with their parents, and 7.4% lived in private houses. Moreover, the majority of students were single (94.6%), while a small percentage were married (5%).
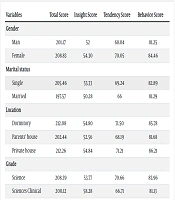
Insight was assessed using 12 questions, with scores ranging from 20 to 60 and an average score of 53.16. Attitude was evaluated through 16 questions, with scores ranging from 24 to 80 and an average score of 69.05. Behavior was measured with 20 questions, yielding scores between 44 and 100 and an average score of 81.82. The total spiritual health score ranged from 88 to 240, with an average score of 205.03 (Table 1).
| Variables | Total Score | Insight Score | Tendency Score | Behavior Score |
|---|---|---|---|---|
| Gender | ||||
| Man | 201.17 | 52 | 68.04 | 81.25 |
| Female | 208.83 | 54.30 | 70.05 | 84.46 |
| Marital status | ||||
| Single | 205.46 | 53.33 | 69.24 | 82.89 |
| Married | 197.57 | 50.28 | 66 | 81.29 |
| Location | ||||
| Dormitory | 212.08 | 54.80 | 71.50 | 85.78 |
| Parents' house | 202.44 | 52.56 | 68.19 | 81.68 |
| Private house | 212.26 | 54.84 | 71.21 | 86.21 |
| Grade | ||||
| Science | 208.39 | 53.77 | 70.66 | 83.96 |
| Sciences Clinical | 200.12 | 58.28 | 66.71 | 81.13 |
The Score Status of Different Areas
Analysis revealed a significant difference between genders only in the realm of insight questions. However, there were no significant differences between single and married students across all areas. Additionally, there were no significant differences between students in basic and clinical sciences, except for orientation questions, where a significant difference was observed. Notably, students living in dormitories differed significantly from those residing with their parents in terms of insight and attitude questions.
5. Discussion
The overall score for spiritual health was 205.03, falling within the lower to average range according to the grading criteria established by the bulletin designers. Analysis of the average scores across different areas revealed that students scored higher in insight and attitude compared to behavior. This suggests that while awareness and attitude are crucial for students' commitment to health components, they alone are insufficient.
Female, single, and dormitory-residing medical students attained higher scores across all three fields. Furthermore, basic science students scored higher than clinical students in all areas. There were no significant differences between single and married students across all areas, nor between basic and clinical sciences regarding orientation questions. However, a significant difference was observed between students living in dormitories and those living with their parents, particularly in insight questions.
Comparing our findings with those of Sayyadi et al., who examined spiritual health levels among students of Kurdistan University of Medical Sciences, Azad Islamic University of Sanandaj, and University of Kurdistan, we find that our students' spiritual health ranged from moderate to high. This indicates a desirable and appropriate level of spiritual health among our study participants. Additionally, while there was a difference in spiritual health between male and female students, with females scoring higher, the overall difference was not statistically significant (10).
Certainly, variations in reported levels of spiritual health may stem from differences in assessment tools. However, discussing the lack of significant difference between men and women, our findings align with Nasrollahi et al.'s study, which aimed to assess the spiritual health of students at Qom Medical School in 2019. They found that students scored higher in vision and attitude compared to performance. Notably, no statistically significant difference was observed between the average scores of spiritual health among male and female groups, as well as between native and non-native students. This parallels the outcomes of our study, where there was no significant difference in spiritual health scores across various dimensions and residency statuses, despite women scoring higher overall (27).
This trend is consistent with research conducted by the WHO (2006) regarding women's understanding of spiritual communication. In our study, we found no significant relationship between spiritual health and native or non-native status. However, we did observe a significant difference in spiritual health scores between native students (residing with parents) and non-native students (residing in dormitories) (27).
On the other hand, Rahimi et al. reported higher levels of spiritual health (28), whereas Rahimi et al.'s studies in Kerman, as well as Rehman et al.'s study, found that women exhibited greater spiritual health (22).
Ebrahimi et al., in a study titled "Comparison of mental health and components of positive psychology in medical students of Isfahan University of Medical Sciences in terms of years of study and relationship with academic progress," found that spirituality, as one of the components of positive psychology, is lower in non-native students compared to native students (29). Tavan et al.'s study indicated that family plays a decisive role in students' spiritual health, particularly when they are with their families (30). Additionally, Sotoodeh et al.'s research suggests that family health significantly contributes to individuals' spiritual well-being (31).
Borna et al., in their study aimed at determining the relationship between spiritual health and academic progress among students of Bushehr University of Medical Sciences, found that most individuals had an average level of spiritual health (32). They also observed a significant relationship between spiritual health and gender, with girls scoring higher than boys. Furthermore, they noted that spiritual health tends to decrease with increasing age and years of education. Additionally, they found a significant relationship between students' spiritual health and their fathers' education level, highlighting the influential role of parents on their children's spiritual health and academic and social performance.
Moreover, dormitory students exhibited better spiritual health status. This could be attributed to the challenges and experiences students face during their studies, especially non-native students who encounter difficulties due to being away from their families, parental guidance, travel, and living in dormitories, all of which can impact their academic performance and spiritual well-being.
The high level of spiritual health observed among students living in dormitories may be attributed to the challenges they face, fostering a sense of need, as well as the availability of religious and ritual facilities in the university and dormitory environments, which attract non-native students. Based on the obtained results, it can be argued that spirituality transcends gender boundaries, as the scores for spiritual health are nearly identical between both sexes (32). This finding underscores the importance of incorporating spiritual education into medical curricula to mitigate gender-related biases in outcomes. It is hoped that integrating spirituality-related curriculum into medical education, particularly in the seven-year medical course, will contribute to enhancing students' overall health.
Using Amiri et al.'s Spiritual Health Questionnaire, spiritual health was assessed across three components: Insight, attitude, and performance (26). While higher scores were achieved in the insight and attitude components compared to performance, this trend was consistent across all groups studied (native and non-native, male and female). The lower performance scores in the insight and attitude components suggest that mere awareness of spirituality does not necessarily translate into practical commitment. The relatively low scores in the functional dimension of spiritual health highlight the need for targeted efforts to promote action and behavioral manifestation, alongside enhancing students' insight.
Research conducted by Ajdarifard et al. on individuals involved in education demonstrated that teaching spiritual concepts to young people significantly impacts the practical aspect of their mental health (33). Many young people relocate from their families due to their studies, facing psychological pressures associated with adapting to dormitory life and academic demands. Medical students, particularly in clinical settings, encounter additional stresses that can impact their efficiency and academic performance, potentially leading to academic challenges. Numerous studies have established a significant relationship between positive components such as happiness and hope and spirituality, underscoring the importance of spiritual well-being in mental health (34, 35).
5.1. Conclusions
The overall score for spiritual health was found to be at a lower level, with higher average scores observed in the areas of insight and attitude compared to performance. Based on the findings of this study, it is anticipated that policymakers and educators in medical programs will enhance spiritual health among students by effectively formulating and implementing educational strategies that incorporate spiritual content and themes, fostering a conducive learning environment, and providing suitable spiritual role models. These efforts aim to cultivate students' insight, attitude, and performance throughout their academic journey.
