Different drugs and diverse anesthesia techniques are used for pediatrics anesthesia in radiotherapy for ensuring immobility and sedation during this procedure, such as inhalation anesthesia (
17); intramuscular and intravenous methohexital (
18,
19); oral, intramuscular, and intravenous ketamine (
19,
20); intravenous thiopental (
21); intravenous meperidine; intravenous midazolam, and oral chloral hydrate (
22). However, in recent years, propofol has become the standard anesthesia care for radiation therapy in children (
23-
25). In our study, we utilized multiple techniques and drugs. This study was conducted in a restricted area with specific demographic and genetic characteristics.
Sedation and anesthesia techniques were used in four stages: minimal sedation, moderate sedation, profound sedation, and general anesthesia with minor or major complications attached to them, especially in pediatrics with brain tumors. Several studies demonstrated anesthesia-related neurotoxicity when pediatrics undergo radiation therapy and receive multiple anesthesia (
26-
28).
There was no statistically significant relationship between age, gender, weight, and complications in this study. Same studies showed similar results (
29,
30). In Owusu-Agyemang et al.’s study conducted on 340 pediatric undergoing radiotherapy, 9,328 inductions by TIVA (total intravenous anesthesia) were performed using propofol and, if necessary, dexmedetomidine and narcotic with complication incidence of 0.05%, including desaturation, seizure, laryngospasm, and bronchospasm (
31).
In a prospective study, 26 institutions conducted 30,037 anesthetic/sedation inductions that demonstrated the overall incidence of complications of 5.3%. Cardiac arrest occurred once, oxygen desaturation below 90% for > 30 seconds occurred 471 times, and stridor and laryngospasm happened 13 times. Unexpected apnea, excessive secretions, and vomiting frequencies were 72, 125, and 142, respectively (
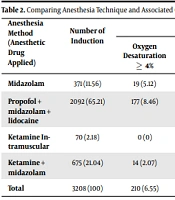
32). Our study did not have any significant anesthesia complications, such as laryngospasm, aspiration, bronchospasm, stroke, arrhythmia, tachyphylaxis, and death. Minor complications were mainly related to the brain tumor's location, procedure duration, and previous chemotherapy that caused peripheral venous damage. Thus, the anesthesia technique was modified from intravenous approach to Intra muscle technique (IM ketamine).
Complications of ketamine-based anesthesia in children radiotherapy were 23 - 24% in previous studies, comprising inadequate movement control, sialorrhea, and slow recovery (
7,
33). Furthermore, ketamine had the highest number of complications in a recently conducted review with a 24% overall rate (
7,
33). Our study used ketamine intramuscular, and ketamine + midazolam was the leading cause of delay in consciousness return, insufficient motionlessness, nausea, vomiting, and patient discharge from the recovery.
Using intramuscular ketamine was due to the inability to obtain an intravenous line related to peripheral venous phlebitis due to chemotherapy. However, some studies stated that chemotherapy does not seem to add the appreciable risk of complications except neutropenic sepsis (
22). On the other hand, using more recent medications such as propofol was lower. A study conducted 1,033 consecutive sedations in children radiotherapy; the overall complication rates were from 0.01 to 3.5% (
22). Thus, based on the data available in this study, propofol + midazolam + lidocaine combination for anesthetizing children as sedatives have been associated with minor complications compared to other utilized anesthesia or sedation methods.
The difference between the incidence of complications in our study and other cited studies is the definition of desaturation, generally described as a decrease in the mean oxygen saturation of ≥ 4% that lasts for at least 10 seconds (apnea ≥ 10 (S)).
The present study showed a significant relationship between the tumor location, procedure duration, anesthesia, and neurologic complications. Anghelescu et al. found four factors that were significantly associated with the risk of complications: duration of the procedure, the total dose of propofol, anesthesia with propofol plus adjunct agents (as compared to propofol alone), and simulation (as compared to radiation treatment) (
29).
5.1. Conclusions
Anesthesia is just one of many factors suggested to play a role in pediatric complications with a brain tumor. Anesthesia complications in the present study were minor and trivial. Furthermore, some of them were due to the tumor effect on other vital organs and previous radiotherapy or chemotherapy. To provide safe anesthesia, considering tumor effects on body organs and neurologic complications caused by it to reduce the anesthesia complications in pediatrics under radiotherapy can be very helpful and practical. The safest anesthetic needs to lie within the anesthesia provider, examining the patient and reviewing the patient’s past medical history. Consequently, the anesthesia team and radiation oncologists must keep up to date with the current knowledge and evidence in this area.
5.2. Suggestions
Conducting more research in this field and a combination of clinical knowledge and experience to generalize the results of evidence-based studies are suggested.