Glioma is one of the most common malignant brain tumors, accounting for more than half of intracranial tumors. PTBE is a common complication of gliomas. The mechanism of PTBE is very complex, although most studies have implicated changes in vascular permeability, increased aquaporins, and cytotoxic factors as significant etiological factors (
12,
13). Some scholars (
5,
14) have observed that the degree of PTBE is positively related to the malignancy grade of glioma; in other words, the degree of PTBE often increases with the malignancy grade of tumor.
Tumor cells often infiltrate into the area of PTBE, probably because the presence of PTBE loosens the peritumoral tissue, which is beneficial for the growth and diffusion of tumor (
15). In this regard, a previous study revealed that the degree of glial PTBE in the human brain was associated with the pathological grade and Karnofsky score, while it was independent of tumor size or shape (
14). Therefore, further elaboration of the relationship between the pathological type of glioma and PTBE can be helpful for clinical diagnosis and treatment.
Some studies have revealed that the degree of PTBE in patients with gliomas is associated with the tumor grade. A previous study showed that the PTBE of patients with grade III-IV gliomas was significantly higher than that of patients with grade I-II gliomas (
16). In other words, the more malignant the tumor cells are, the more immune-related and inflammatory factors, such as vascular endothelial growth factor, prostaglandin, vascular endothelial growth factor, nitric oxide synthase, and arachidonic acid, are secreted, changing the permeability of the blood-brain barrier and aggravating brain edema. Simultaneously, HGGs grow faster, and the presence of PTBE further compresses the surrounding brain tissue and blocks the venous reflux of the surrounding tissue, aggravating the degree of PTBE (
17,
18).
In recent years, some scholars have suggested that neovascularization lacks a complete blood-tumor barrier and that some neovascularization may derive from the transformation of tumor stem cells (
19,
20). By evaluating the relationship between preoperative edema degree and benign and malignant gliomas through MRI, the present study proved that the difference in the degree of EI between benign and malignant gliomas was significant and that the degree of PTBE was positively correlated with the malignant degree of glioma. Overall, our study provided an imaging reference for rapid preoperative differentiation of benign and malignant gliomas.
In the present study, we calculated EI as our main objective rather than the edema volume to determine whether the malignancy grade of tumor can be determined by the volume of PTBE rather than only the volume of tumor; the present results confirmed the value of this parameter. Other studies of glioma grading suggest age as an individual differentiating factor between LGGs and HGGs, unlike gender (
21,
22). However, in the present study, the value of age was not significant, we look forward to a multicenter and big sample research to further confirm it.
Ki-67 is a proliferating cell-associated nuclear antigen, which is involved in all active stages of the cell cycle, but not in the resting stage. Ki-67 has been used as a biomarker for expressing the proliferative activity of tumor cells (
16) to provide information on the tumor biological behavior, therapeutic response, and prognosis (
23). In this regard, Su et al. (
24) observed that the Ki-67 expression in LGGs was significantly lower than that of HGGs. Therefore, the degree of malignancy increased with the grade of glioma. Moreover, Bai et al. (
25) observed that Ki-67 can distinguish between not only HGGs and LGGs, but also between grade III and IV gliomas. However, Skjulsvik et al. (
9) argued that Ki-67 has limited potential to distinguish between LGGs and HGGs. Therefore, it cannot be used as an independent marker of glioma grading and should be combined with histological features. Nevertheless, it was confirmed that Ki-67 can be useful for grading gliomas.
Although Ki-67 is useful for grading and malignancy assessment of gliomas, its measurement requires either biopsy or surgical resection and is affected by errors of heterogeneous tumor sampling, limiting its diagnostic accuracy, especially in small samples, such as stereoscopy (
9). Therefore, non-invasive prediction of Ki-67 expression in different tumor regions is of great importance. In our study, evaluating the relationship between the degree of PTBE and the preoperative Ki-67 expression, the degree of PTBE was positively correlated with the Ki-67 expression level. Therefore, Ki-67 not only can evaluate the proliferative activity of gliomas, but also has some correlations with imaging parameters, which is significant for the non-invasive evaluation of malignancy.
The IDH1 mutation status is significant in the occurrence and progression of gliomas and is expected to be a key target in future therapies (
26). The IDH1 mutant tumor cells are susceptible to oxidative damage during radiotherapy and chemotherapy, making the treatment more effective and increasing the patient survival (
27,
28); therefore, predictive IDH1 typing is crucial for clinical decision-making. The present study demonstrated that the degree of PTBE has a significant difference between IDH wild and mutation type, but it was not a independent factor for prediction of IDH1 statue (P > 0.05), indicating that PTBE might not be used as a predictive factor for patients' survival.
MRI has become the main imaging modality for the non-invasive evaluation of the malignant grade of gliomas. Multimodal MRI sequences can further improve the accuracy of predictions. Although our study exhibited a correlation between PTBE and certain glioma characteristics, it had some limitations. First, because the sample size was not large enough, more patients from multiple centers were needed to confirm the generalizability of our model to overcome the limitation of population bias in this retrospective study. Second, measurement of edema was not accurate enough, and more advanced technologies and tools are needed to refine it.
Third, not all preoperative sequences were considered for every patient, and other important MRI sequences, such as diffusion-weighted imaging and diffusion-tensor imaging, were not included; therefore, further research with prospective multi-parametric MRI scan is needed. Finally, it is difficult to distinguish reactive and infiltrative edemas by MRI, and more attention must be paid to this limitation.
In conclusion, the degree of PTBE can be valuable for differentiating HGGs from LGGs and may be associated with the IDH1 mutation status and Ki-67 expression level. Moreover, the degree of PTBE was positively correlated with the patient’s age, and Ki-67 expression level. Overall, with the introduction of multimodal sequences and parameters, PTBE may be considered a vital, novel, and non-invasive evaluation method of gliomas in the future.
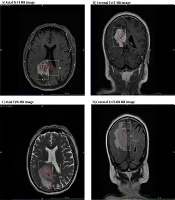



 and tumor + peritumoral brain edema (PTBE) (C and D); tumor region is referenced to the T1-CE image, while PTBE is referenced to the T2WI or T2-FLAIR image. A1, B1, and C1 represent the maximum diameters of the measured tumor volume in the axial, sagittal, and coronal aspects of the tumor, respectively. A2, B2, and C2 represent the three maximal diameters of tumor core + PTBE, respectively.")
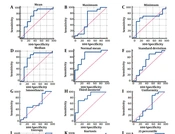
![The receiver operating characteristic (ROC) curve analysis of edema index (EI) for predicting the glioma grade [low grade glioma (LGG) or high grade glioma (HGG)]](https://brieflands.com/journals/ijradiology/articles/109181/figures/iranjradiol-109181-i002-F3-preview.webp "The receiver operating characteristic (ROC) curve analysis of edema index (EI) for predicting the glioma grade [low grade glioma (LGG) or high grade glioma (HGG)]")